
Because the duration is short and the clearance is relatively low, RKF contributes little to the decrease in BUN levels during dialysis. The effect of residual urea clearance (Kr) is seen during the long interdialysis interval when it serves to decrease the predialysis BUN level, as shown in Fig 6. When Kr is zero, the interdialysis rise in the BUN level is linear in the absence of fluid gain. If Kr is greater than zero, the increase in BUN level between dialyses is curvilinear and concave downward, resulting in a lower predialysis BUN level, so less HD is required to maintain the same average BUN level.
Fig 6. Effect of residual native kidney clearance (Kr). The increase in BUN levels from the post-BUN level to the next pre-BUN level is modulated by Kr, as shown in the lower curve. The result is a pre-BUN level that is lower when compared to the pre-BUN level in the absence of Kr (upper line).
In addition, the continuous nature of Kr provides a more efficient clearance, so simply adding the time-averaged Kr to time-averaged Kd underestimates the contribution of Kr to overall clearance. A quantitative relationship between Kr, Kd, and overall urea clearance can be developed by applying a mathematical model of urea kinetics. The goal is to determine how much of a decrease in Kd can be allowed to achieve the same level of BUN when Kr is added. The following simplified formula depicts the relationship between dialyzer clearance (Kd) in the absence of Kr, and lower dialyzer clearance (Kd´) permitted in the presence of Kr.360,361
![]()
Kr, Kd and Kd´ are expressed in milliliters per minute; t is the duration of HD in minutes.
In this formula, k relates Kr to the difference between Kd and Kd´, or the decrease in dialysis dose that is possible while still achieving the same BUN level that would be expected when there is no Kr. The parameter k has units of mL/(mL/min) and when multiplied by Kr permits an expression of Kr in equivalent dialysis units than can be spared. It can also be considered as a time or duration of Kr analogous to dialysis duration (t), but always is higher than the average interval between dialyses (ti) because Kr is more efficient than Kd. When expressed per dialysis, the relationship among the reduced dialysis dose (Kd´t/V), the required dose in the absence of Kr (Kdt/V), and the residual native kidney clearance (kKr/V), is expressed by:
![]()
where V is the patient's volume of urea distribution in milliliters.
In the absence of kinetic modeling, Kd´t/V can be solved by substituting the interdialysis interval (10,080 min per wk/frequency) for k in this expression. Note that this approach, shown in the first data column in Table 18, ignores the improved efficiency of the continuous RKF, but it is considered safe for the patient because it underestimates the effect of Kr.
Another method to incorporate Kr into Kt/V is based on the equivalent clearance (EKR),264 which represents the continuous equivalent of the patient's intermittent urea clearance and can be calculated as follows:

The result can be normalized to a typical V of 35 L and expressed in terms of nPCR and TAC using the equation for nPCR.362
![]()
EKR is a total clearance that includes RKF, but the dialyzer component can be extracted by subtracting Kr. EKR is the continuous clearance necessary to maintain the equivalent TAC at the patient's nPCR. The EKR of intermittent HD can be directly compared to the EKR of patients dialyzed at any frequency or with the clearance of continuously functioning native kidneys. Routinely solving these equations requires the use of computational software.
The use of EKR has been criticized because it fails to fully account for the improvement in efficiency associated with the continuous clearance of native kidneys or continuous dialysis. 267 Apparently, equating average urea concentrations ignores other more toxic solutes for which the difference in removal by continuous compared with intermittent clearance is greater than for urea. Equating “standard clearances” using the average peak BUN instead of TAC in the previous equation has been offered as a solution to this apparent problem.265
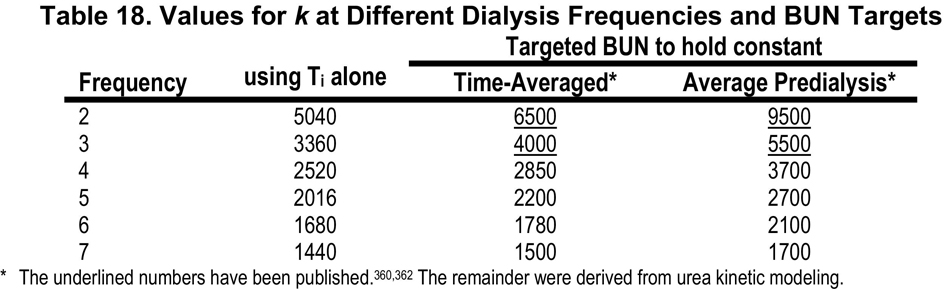
Instead of inflating Kr to match the relatively inefficient non-continuous dialyzer clearance as described above, an alternative method, favored by the Work Group, reduces the dialyzer clearance to a continuous equivalent clearance, based on normalizing the predialysis BUN. This continuous equivalent of a dialyzer clearance, also known as “standard clearance”265 (stdK) is the continuous clearance that maintains the BUN at a constant value equal to the average predialysis BUN achieved during intermittent dialysis. Because the pre-dialysis BUN is targeted, this approach gives results similar to that depicted in the third data column of Table 18. After normalizing the dialyzer clearance to stdK, Kr can simply be added to it because both can be considered continuous clearances. Dialyzer clearances (spKt/V) required to achieve a stdKt/V of 2.0 volumes per week are shown in Table 19 for treatment times that vary from 2 to 8 hours and for schedules from 2 to 7 treatments per week. These values were determined using a formal 2-compartment mathematical model of urea kinetics but similar results are obtained using the simplified equation for stdKt/V shown in section CPR2.
