8.1 Choice of access type:
- 8.1.1 Permanent access in the form of a fistula or graft is the preferred form of vascular access for most pediatric patients on maintenance HD therapy.
- 8.1.2 Circumstances in which a CVC may be acceptable for pediatric long-term access include lack of local surgical expertise to place permanent vascular access in small children, patient size too small to support a permanent vascular access, bridging HD for PD training or PD catheter removal for peritonitis, and expectation of expeditious kidney transplantation.
- 8.1.3 If surgical expertise to place permanent access does not exist in the patient's pediatric setting, efforts should be made to consult vascular access expertise among local adult-oriented surgeons to either supervise or place permanent vascular access in children.
- 8.1.4 Programs should evaluate their patients' expected waiting times on their local deceased-donor kidney transplant waiting lists. Serious consideration should be given to placing permanent vascular access in children greater than 20 kg in size who are expected to wait more than 1 year for a kidney transplant.
8.2 Stenosis surveillance:
An AVG stenosis surveillance protocol should be established to detect venous anastomosis stenosis and direct patients for surgical revision or PTA.
8.3 Catheter sizes, anatomic sites, and configurations:
- 8.3.1 Catheter sizes should be matched to patient sizes with the goal of minimizing intraluminal trauma and obstruction to blood flow while allowing sufficient blood flow for adequate HD.
- 8.3.2 External cuffed access should be placed in the internal jugular with the distal tip placed in the right atrium.
- 8.3.3 The BFR of an external access should be minimally 3 to 5 mL/kg/min and should be adequate to deliver the prescribed HD dose.
Applicability of Previous KDOQI Vascular Access Guidelines to Pediatric Patients
Provision of validated evidence-based pediatric vascular guidelines is hampered by a number of pediatric CKD stage 5–related epidemiological issues. Most of the recommendations outlined in the first edition of the KDOQI Vascular Access Guidelines are pertinent to pediatric patients, although few published data exist to support more than opinion-based recommendations. Some pediatric HD vascular access descriptive and comparative clinical research has been conducted since the first edition of the KDOQI Vascular Access Guidelines, which provide data to formulate a first set of both evidence- and opinion-based recommendations for children receiving maintenance HD. Rather than restating the previous CPGs in their entirety with annotation of the few areas in which the emphasis may be different for pediatric patients, we have opted to present separate pediatric Vascular Access Guidelines based on the available pediatric literature. For specific vascular access areas not addressed in these pediatric guidelines, the practitioner should refer to the relevant adult KDOQI Guidelines.
Choice of Access Type (CPR 8.1)
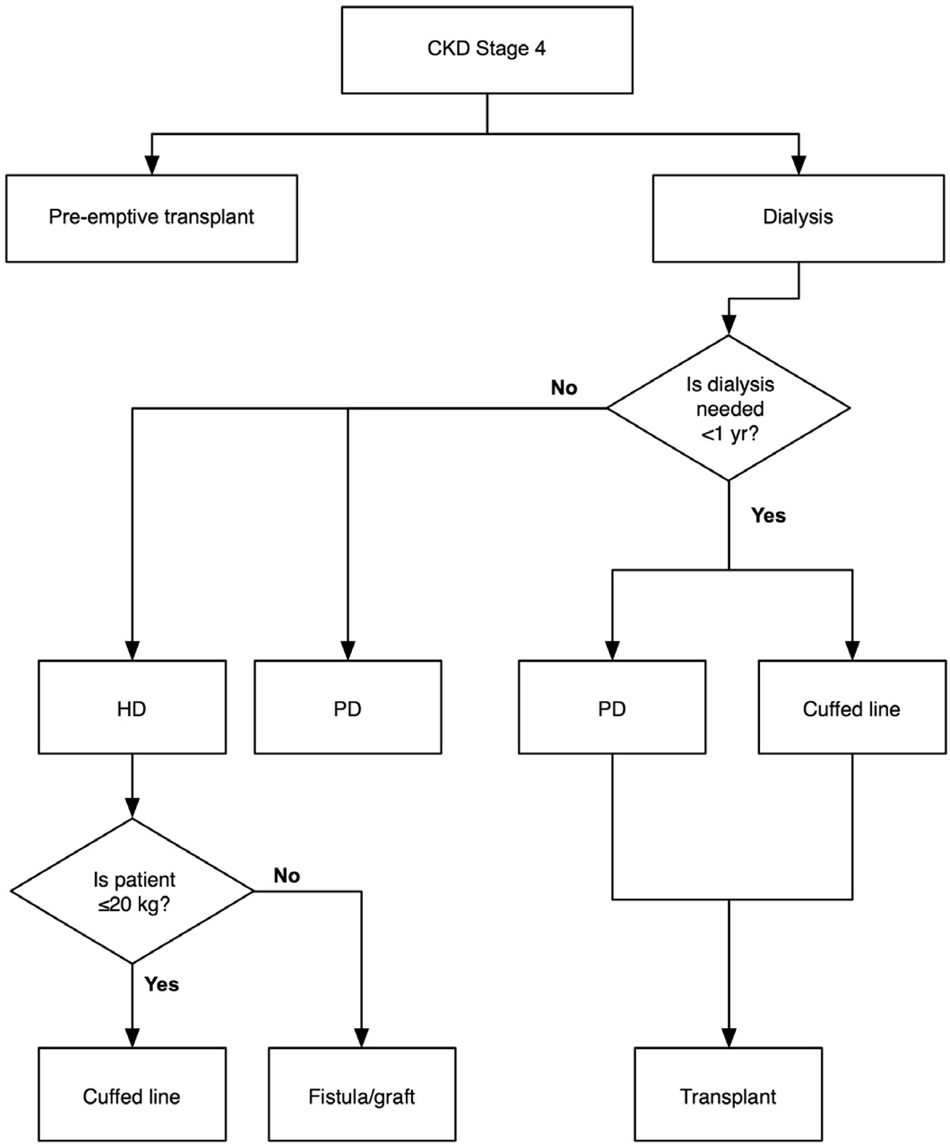
Kidney transplantation remains the preferred and predominant therapy for pediatric patients with CKD stage 5; therefore, many pediatric patients receive maintenance HD through an indwelling catheter in light of short deceased-donor waiting list times or a readily available living-related donor (see Fig 11).610 Because fewer than 800 pediatric patients receive maintenance HD therapy in the United States, surgical expertise for placing fistulae or grafts in small patients may be limited by the infrequent need and sporadic caseload. Smaller patients, especially those less than 10 kg, present technical challenges in terms of both surgical and nursing skill; therefore, the majority of smaller patients receive PD for their maintenance dialysis modality.
Fig 11. Pediatric progress from CKD stages 1 to 5 and KRT/access algorithm.
Recent data show that AVFs and AVGs typically function longer75,611-613 than catheters614-616 in pediatric patients receiving maintenance HD therapy. Functional survival rates of AVFs and AVGs are similar to adult patient standards and those recommended by KDOQI Vascular Access Guidelines, with centers recently reporting 4-year functional survival rates of 40% to 60%. Despite this, the most recent CMS CPM and North American Pediatric Renal Transplant Cooperative Study data617 show that 62% to 78% of pediatric maintenance HD patients have catheters as their vascular access. While reports of successful permanent vascular access in children less than 10 kg in size exist,611,612,618 maturation can take up to 4 to 6 months, making routine permanent access placement impractical in many pediatric situations. Since the late 1970s, both AVFs and AVGs have been placed in children requiring maintenance HD.619 The major complications of pediatric fistulae include a primary nonfunction rate of 20% to 33%, usually because of lack of maturation or clotting. Pediatric fistulae can develop stenosis anywhere along the fistula, most of which is amenable to either surgical correction or PTA.620 Given the relatively long life expectancy for pediatric patients with CKD stage 5 (79% at 10 years and 66% at 20 years),621 all efforts should be made to use distal sites for initial fistula creation, ie, the radiocephalic fistula configuration. For patients less than 10 kg in size with a creatinine clearance between 20 and 25 mL/min/1.73 m2 in whom imminent dialysis is not required, microsurgical techniques should be used for fistula creation.611,612 Fistulae in smaller children may require 4 to 6 months for adequate maturation.
Stenosis Surveillance (CPR 8.2)
AVGs offer the advantage of more flexible surgical configurations, which include the use of thigh vessels. Recent data show that AVGs can function well in pediatric patients receiving maintenance HD, with functional survival rates similar to adult patient standards and KDOQI Vascular Access Guidelines.613 As with AVFs, the more distal anatomic sites should be used for first access to preserve more proximal sites for access in later life. AVG venous outflow stenosis predisposes pediatric patients to AVG thrombosis. Recent pediatric data show that UDTs are very sensitive to predict venous stenosis.365 A proactive ultrasound dilution venous stenosis assessment protocol directing patients to angioplasty with a corrected access flow less than 650 mL/min can lead to a significant decrease in AVG thrombosis rates.622,623 One pediatric study found that static venous pressure monitoring did not help in the diagnosis of venous stenosis.624 No data exist about the long-term effect of decreased thrombosis rates on AVG survival in children.
Catheter Sizes, Anatomic Sites, and Configurations (CPR 8.3)
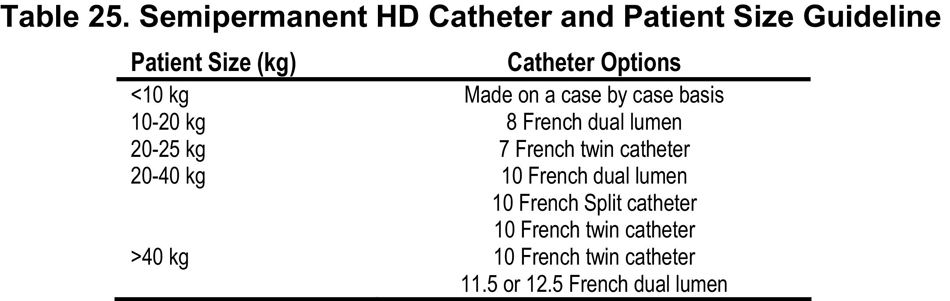
The choice of catheter size and configuration depends on the size of the patient. Studies to date suggested that children as small as 4 to 5 kg can tolerate dual-lumen 8 Fr catheters, and as the child becomes larger in size, a larger volume access can be placed.625 Table 25 serves as a guideline for matching catheter size to patient size. Choices often are limited based on availability, but considerations should include flow characteristic, recirculation risk, and ease of placement. Data suggest that for the appropriately sized patient, twin single-lumen catheters (the Tesio System) may provide better performance than standard dual-lumen catheters.616 Longer and more narrow catheters result in greater resistance to flow.626
Catheter placement considerations in pediatrics are similar to those in adults, with a preference for internal jugular veins over subclavian veins. Right atrial placement may prevent inlet or outlet hole occlusion by blood vessels and thus allow for the high flow rates needed to provide adequate dialysis. Data have suggested that subclavian stenosis occurs in excess of 80% of patients in pediatrics who have subclavian catheters (Denis Geary, personal communication). Femoral access can be used when upper-anatomy venous access is no longer available.627
Flow rates for vascular access should be sufficient to result in a Kt/V greater than 1.2. Kt/V is influenced further by the recirculation rate. Because flow rates in pediatrics vary by the size of catheter, which varies by the size of the patient, a recommended flow rate of 3 to 5 mL/kg/min is acceptable in most patients.628