THE PURPOSE OF this section is to review the general state of knowledge at the start of the Work Group. This review will provide a detailed framework for the questions the Work Group chose to ask.
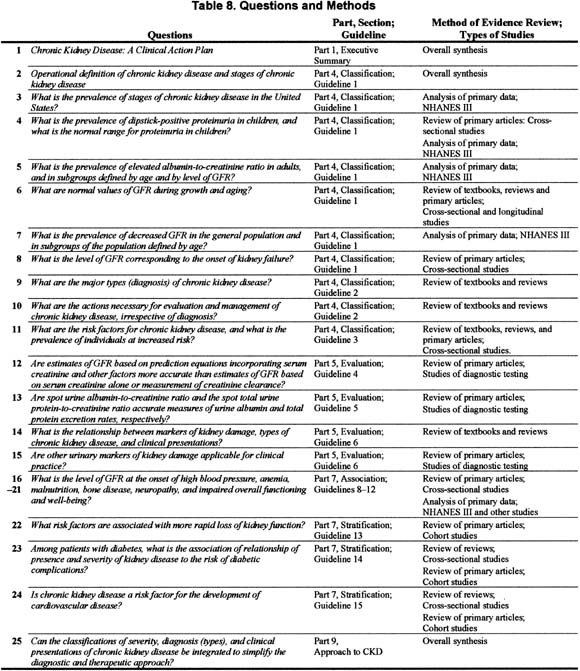
Solutions to public health problems require strategies for prevention of adverse outcomes of disease. Prevention requires a clear understanding of prevalence and outcomes of disease, earlier stages of disease, antecedent risk factors, and appropriate treatments for populations at risk. There is a spectrum of risk for adverse outcomes, ranging from “very high risk” in those with the disease, to “high risk” in those with risk factors for developing the disease, to “low risk” for those without the disease or its risk factors. The population as a whole includes many more individuals at low risk than at high risk. Public health measures addressing chronic diseases include strategies to prevent adverse outcomes in individuals at very high risk and high risk, as well as widespread adoption of life-style modifications to reduce the average risk profile of the population.
With regard to risk stratification for adverse outcomes from chronic kidney disease, patients with chronic kidney disease would be included in the “very high risk” group. Individuals without chronic kidney disease, but with risk factors for chronic kidney disease (“CKD risk factors”), would constitute the “high risk” group. Individuals without chronic kidney disease or CKD risk factors would constitute the “low risk” group.
Most chronic kidney diseases tend to progress and worsen over time. The risk of adverse outcomes in chronic kidney disease can be further stratified by the severity of disease and rate of progression. Therefore, for most patients, the risk of adverse outcomes tends to increase over time.
The major task of the Work Group was to develop “A Clinical Action Plan” — an approach to chronic kidney disease that relates stages of severity of chronic kidney disease to strategies for prevention and treatment of adverse outcomes.
To accomplish this task it was first necessary to outline the conceptual approach, including operational definitions of chronic kidney disease and the stages of severity of chronic kidney disease; determination of the prevalence of chronic kidney disease; issues in the evaluation and management of various types of chronic kidney disease; definition of individuals at increased risk of chronic kidney disease; definition of outcomes of chronic kidney disease; association of complications of chronic kidney disease with decreased kidney function; modalities of kidney replacement therapy; and an approach to chronic kidney disease using the guidelines.
The USRDS provides reliable nationwide data regarding the incidence, prevalence, treatment patterns, outcomes, and cost of the end-stage renal disease, the most severe stage of chronic kidney disease. There are no uniform definitions of earlier stages of kidney disease, nor is there reliable information on the prevalence, treatment patterns, outcomes, and cost of these earlier stages, nor information on how many people choose to forego dialysis and transplantation despite kidney failure. Risk factors for the development of chronic kidney disease have not been well described, and there is no reliable estimate of the size of the population at risk. This section introduces the rationale for developing a definition of chronic kidney disease and classification of stages of severity; risk factors for adverse outcomes of chronic kidney disease; the relationship between disease severity and rate of progression as risks for adverse outcomes; the definitions and stages defined by the Work Group; and laboratory tests for the detection of each stage.
Rationale for Developing a Definition of Chronic Kidney Disease and Classification of Stages of Severity
Defining chronic kidney disease and classifying the stages of severity would provide a common language for communication among providers, patients and their families, investigators, and policy-makers, and a framework for developing a public health approach to affect care and improve outcomes of chronic kidney disease. A uniform terminology would permit:
Clinical practice guidelines, clinical performance measures, and continuous quality improvement efforts could then be directed to stages of chronic kidney disease.
Defining chronic kidney disease and stages of severity requires “categorization” of continuous measures of markers of kidney damage and level of kidney function. Identifying the stage of chronic kidney disease in an individual is not a substitute for diagnosis of the type of kidney disease or the accurate assessment of the level of kidney function in that individual. However, recognition of the stage of chronic kidney disease would facilitate application of guidelines, performance measures, and quality improvement efforts.
In other fields of medicine, classifications of stages of severity of illness have been adopted with apparent success, such as the New York Heart Association classification of heart disease. Within nephrology and related disciplines, classifications of disease severity have been developed that are based on “categorization” of continuous measures of disease severity. For example, the Joint National Committee for the Prevention, Detection, Evaluation and Treatment of High Blood Pressure has defined stages of hypertension based on blood pressure level. The National Cholesterol Education Program has defined stages of hypercholesterolemia based on serum cholesterol level. Diabetic kidney disease is classified according to the magnitude of albuminuria. Criteria for enrollment into the Medicare ESRD Program and “listing” for cadaveric kidney transplantation are based, in part, on the level of serum creatinine. These classifications have facilitated epidemiological studies, clinical trials, and application of clinical practice guidelines.
Risk Factors for Adverse Outcomes of Chronic Kidney Disease
A risk factor is defined as an attribute that is associated with increased risk of an outcome. In principle, there are four kinds of risk factors for adverse outcomes of chronic kidney disease which were defined by the Work Group as “CKD risk factors” (Table 9).
This guideline concerns itself primarily with identifying susceptibility and initiation factors to define individuals at high risk of developing chronic kidney disease, and with progression factors, to define individuals at high risk of worsening kidney damage and subsequent loss of kidney function.
Relationship Between Disease Severity and Rate of Progression as Risks for Adverse Outcomes
In principle, one may distinguish between the severity of disease and the risk for adverse outcomes of disease. The severity of disease can be determined from measurements of level of organ function, complications in other organ systems, morbidity (symptoms and clinical findings), and impairment in overall function and well-being. In general, the risk for adverse outcomes is related to the severity of disease. In addition, the risk for adverse outcomes is also dependent on the rate of progression to a more severe stage or the rate of regression to a less severe stage.
For the case of chronic kidney disease, these concepts can be illustrated by Fig 4.
Figure 4 |
|
Kidney function decline in chronic kidney disease. See text. |
|
The vertical axis shows the level of kidney function. The horizontal axis shows time over an interval of several years. The horizontal dotted line corresponds to the level of kidney function at the onset of kidney failure. The declines in kidney function in 4 individual patients (A through D) are illustrated as diagonal lines. At the discovery of chronic kidney disease (t0), patients A and B share identical levels of kidney function, as do patients C and D, but the level of function is lower in patients C and D than for patients A and B. Patients A and C have identical rates of decline in kidney function, as do patients B and D, but the rate of decline is faster in patients B and D than in patients A and C. Patient D, with the lower initial level of kidney function and the faster rate of decline in kidney function, reaches kidney failure first (t1). Patient B, with the higher initial level of kidney function but faster rate of decline, and patient C, with the lower initial level of kidney function and slower rate of decline, reach kidney failure at the same time (t2). Patient A, with the higher initial level of kidney function and the slower rate of decline in kidney function, has not reached kidney failure by the end of follow-up (t2). Figure 4 illustrates that the risk of developing kidney failure depends both on the level of kidney function at the discovery of chronic kidney disease and the rate of decline in kidney function. The object of therapy for chronic kidney disease would be to detect kidney disease at a higher level of kidney function (open arrow) and to reduce the rate of decline in kidney function thereafter (filled arrows), thereby reducing adverse outcomes of chronic kidney disease.
Operational Definition of Chronic Kidney Disease and Stages
One of the first tasks of the Work Group was to define chronic kidney disease, irrespective of the specific pathological features of the disease. For this definition, the Work Group used a combination of the presence of kidney damage and level of kidney function.
Definition and Detection of Kidney Damage
Chronic kidney damage is defined as structural abnormalities of the kidney that can lead to decreased kidney function. The level of glomerular filtration rate (GFR) is accepted as the best measure of overall kidney function in health and disease. Pathologic studies show that substantial kidney damage can be sustained without decreased GFR. Micropuncture studies in animal models of chronic kidney disease show that the maintenance of normal GFR despite kidney damage is due to an adaptive increase in glomerular capillary blood flow and pressure in response to decreased ultrafiltration coefficient and reduced number of nephrons.
Markers of kidney damage vary depending on the type of kidney disease and may include abnormalities in the composition of the blood or urine or abnormalities in imaging tests, with or without decreased GFR. For example, albuminuria is widely accepted as a marker of glomerular damage, and the excretion of even small amounts of albumin (microalbuminuria) is the earliest manifestation of diabetic kidney disease. In large amounts, albumin excretion can readily be detected by tests of total urine protein, whereas detection of minimal amounts requires specific, sensitive assays.
One of the major obstacles to detection of kidney damage using measurements of urine albumin or total protein is the necessity for collection of a timed urine sample. Recently, many investigators have provided evidence that the ratio of concentrations of albumin-to-creatinine or total protein-to-creatinine in a spot urine sample accurately reflects the excretion rates of albumin or total protein in timed urine samples. One of the questions posed by the Work Group was: Do spot urine albumin-to-creatinine ratio and total protein-to-creatinine ratio provide accurate measures of urine albumin and protein excretion rates, respectively?
In addition to its importance as a marker of kidney damage, albuminuria is also an important prognostic factor for the progression of kidney disease and development of cardiovascular disease. The NKF issued a position paper in 1999 on the evaluation and management of adults with albuminuria. The initiative, known as “Proteinuria, Albuminuria, Risk Assessment, Detection, and Elimination (PARADE),” emphasizes findings related to proteinuria as a risk factor for cardiovascular disease, proteinuria as a mediator and marker of progressive kidney disease, and persistent massive proteinuria as the inciting factor that leads to the nephrotic syndrome.6 An accompanying report on the evaluation and management of proteinuria and nephrotic syndrome in children was issued in 2000.7 The CKD Work Group has used the recommendations of PARADE in developing its recommendations for laboratory testing and evaluation of proteinuria and albuminuria.
Other examples of markers of damage in chronic kidney disease include abnormalities in the urine sediment and abnormalities on imaging studies of the kidney. One of the questions posed by the Work Group was: Are other urinary markers of kidney damage applicable for clinical practice?
High blood pressure was not defined as a marker of kidney damage because high blood pressure has other causes. The relationship between high blood pressure and kidney disease is complex, as high blood pressure is both a cause and a consequence of kidney disease. Throughout the guideline, the Work Group has provided information on high blood pressure, including the prevalence of high blood pressure at stages of chronic kidney disease, and the role of high blood pressure as a risk factor for loss of kidney function.
Definition and Detection of Decreased GFR and Relationship With Age
As a rule, kidney failure due to chronic kidney disease is preceded by a stage of variable length during which GFR is decreased. GFR is affected by a number of factors in addition to kidney disease, and not all individuals with decreased GFR have chronic kidney disease. Mild reduction in GFR was defined as chronic kidney disease only in the presence of kidney damage (Stage 2). However, because of the risk of complications, moderate (Stage 3) to severe (Stage 4) reduction in GFR and kidney failure (Stage 5) were defined as chronic kidney disease, irrespective of the presence of kidney damage. Other than kidney disease, the most important factor affecting GFR is age. GFR rises during infancy and declines during aging. Therefore, mild reduction in GFR may be “normal” at the extremes of age and, in the absence of kidney damage, is not considered to be chronic kidney disease. A clinical action plan based on the level of GFR requires knowledge of age-associated normal values. One of the questions posed by the Work Group was: What are normal values of GFR during growth and aging?
Unfortunately, measurement of GFR is inconvenient, and in most studies, as in clinical practice, the level of kidney function is estimated from the serum creatinine concentration. This is difficult because a variety of factors other than GFR, including age, gender, race, and body size, affect the serum creatinine concentration. To circumvent these limitations, most clinical texts recommend measuring creatinine clearance to estimate the level of GFR. However, as indicated previously, collection of a timed urine specimen can be difficult. One of the questions posed by the Work Group was: Are estimates of GFR based on prediction equations incorporating serum creatinine as well as these other factors more accurate than estimates of GFR based on serum creatinine alone or measurement of creatinine clearance?
Definition and Detection of Kidney Failure
Most texts define kidney failure as severe reduction in kidney function that is not compatible with life, because its attendant complications become increasing risks for mortality. Individuals at this stage have been said to have “end-stage renal disease” (ESRD) because they require dialysis or transplantation to sustain life. Since 1972, the Medicare ESRD Program has borne 80% of the costs of dialysis and transplantation for approximately 93% of patients in the United States, allowing near universal access to treatment for kidney failure. Indeed, treatment with dialysis or transplantation has become almost synonymous with the diagnosis of chronic kidney failure. Such a definition of kidney failure has obvious operational and administrative advantages. However, it lacks precision. First, patients who have kidney failure may survive for variable periods of time without treatment by dialysis or transplantation. Second, some signs and symptoms of kidney failure appear at higher levels of kidney function that are compatible with long survival. Third, some have advocated “early initiation of dialysis” or “pre-emptive” kidney transplantation prior to the onset of kidney failure. Fourth, many patients living with dialysis or a kidney transplant find the phrase “end-stage” threatening and misleading. Thus, it would be preferable to define kidney failure as a combination of signs and symptoms of uremia and a specific level of kidney function. One of the questions posed by the Work Group was: Is it possible to identify the level of kidney function corresponding to the stage of kidney failure?
As described earlier, the USRDS tracks the prevalence of kidney failure in the United States. One of the questions posed by the Work Group was: What is the prevalence of earlier stages of chronic kidney disease, based on the definitions and methods for measurement discussed above?
Prevalence of Kidney Damage
Guidelines by the American Academy of Pediatricians recommend screening school-age children for proteinuria using the urine dipstick. Therefore, a large number of studies have been conducted to estimate the prevalence of proteinuria in children. One of the questions posed by the Work Group was: What is the prevalence of dipstick-positive proteinuria in children? On the other hand, fewer studies have determined the normal range of proteinuria in children. Another question asked by the Work Group was: What is the normal value for proteinuria in children?
In contrast, current guidelines by the US Preventive Health Services Task Force do not suggest routine screening of adults for proteinuria. Data from two community-based screening programs, the Framingham Study,12 and the Okinawa Study,13 demonstrate an approximately 10% prevalence of dipstick-positive proteinuria in adults. The prevalence was higher in older than younger individuals and higher in women than men. However, there are serious limitations to these studies. First, the urine dipstick is not sensitive to small amounts of albumin, and thus these studies would not have detected most patients with microalbuminuria. Second, neither timed urine collections nor protein-to-creatinine ratios were measured, and thus the dipstick test result was affected by the state of diuresis in addition to the magnitude of proteinuria. Furthermore, at least some of the individuals in these studies with proteinuria also had reduced kidney function. Thus, they provide only a rough guide to the likely prevalence of individuals with kidney damage due to chronic kidney disease. Another question posed by the Work Group was: What is the prevalence of elevated urine albumin-to-creatinine ratio in adults; and in subgroups defined by age and level of GFR?
Prevalence of Decreased GFR
A 1998 report from the third cycle of the National Health and Nutrition Examination Survey (NHANES III), conducted from 1988 to 1994, estimated that 6.2 million individuals over age 12 years had reduced kidney function, defined as a serum creatinine concentration ≥ 1.5 mg/dL1.
Figure 5 |
|
Creatinine distribution: US population age |
|
This represents an almost 30-fold higher prevalence of reduced kidney function compared to the prevalence of ESRD during the same interval. This same report estimated that there were 2.5 million individuals with serum creatinine ≥ 1.7 mg/dL and 800,000 individuals with serum creatinine ≥ 2.0 mg/dL. Because of differences in creatinine generation, the prevalence of elevated serum creatinine varied by age, gender, and ethnicity, with a higher prevalence in older compared to younger individuals, in men compared to women, and in non-Hispanic blacks compared to non-Hispanic whites or Mexican-Americans. As discussed later in this report, these apparently minor elevations in serum creatinine may well reflect substantial decreases in GFR, especially in the elderly. This suggests that the number of individuals with reduced kidney function, defined as reduced GFR, may be much higher than these estimates based on increased serum creatinine levels. One of the questions posed by the Work Group was: What is the prevalence of decreased GFR in the general population and in subgroups defined by age?
Diagnosis of chronic kidney disease is based primarily on etiologic and pathologic classification. Refinements in serologic tests and introduction of percutaneous biopsy technique have led to increasingly sophisticated classifications. Unfortunately, nomenclature has not been standardized, which hampers the development of strategies for prevention and treatment14. It is anticipated that a future Work Group will address the role of kidney biopsy. One of the tasks of the Work Group was to recommend a classification of the types of kidney disease for application of these guidelines.
Another task was to describe the actions necessary for evaluation and management of chronic kidney disease, irrespective of diagnosis. The Work Group recommended that these tasks be grouped as follows: treatment of comorbid conditions, prevention or slowing the loss of kidney function, prevention and treatment of cardiovascular disease, prevention and treatment of complications of decreased kidney function, preparation for kidney failure, and replacement of kidney function (if necessary and desired) by dialysis and kidney transplantation.
Data from the USRDS indicates the incidence of ESRD is disproportionately high among older individuals, certain ethnic minorities, and individuals with hypertension, diabetes, and autoimmune diseases. This suggests that demographic and clinical factors may be risk factors for the development or progression of chronic kidney disease. In addition, individuals with a family history of kidney disease appear to be at higher risk of developing kidney disease. This appears to be true for most types of kidney diseases, suggesting the presence of genes coding for susceptibility factors for the development or progression of kidney disease in general, as well as genes coding for specific kidney diseases, such as autosomal dominant polycystic kidney disease or Alport’s syndrome. Finally, patients who have recovered from an episode of acute kidney failure, whether due to acute tubular necrosis or other parenchymal diseases, may also be at risk of developing chronic kidney disease.
The prevalence of individuals at increased risk for development of chronic kidney disease has not been studied systematically. One of the tasks of the Work Group was to assemble a list of potential CKD risk factors and the prevalence of individuals with these risk factors.
The Work Group considered two major outcomes of chronic kidney disease: loss of kidney function leading to kidney failure and development of cardiovascular disease. Of course, kidney failure is the most visible outcome of chronic kidney disease, and loss of kidney function is associated with complications in virtually every organ system. Cardiovascular disease was considered separately because: (1) cardiovascular disease events are more common than kidney failure in patients with chronic kidney disease; (2) cardiovascular disease in patients with chronic kidney disease is treatable and potentially preventable; and (3) chronic kidney disease appears to be a risk factor for cardiovascular disease.
Loss of Kidney Function
A number of studies have examined factors associated with more rapid loss of kidney function in chronic kidney disease. Some diseases are associated with a faster loss of kidney function than others, while some patient factors are known to predict a faster loss of function, irrespective of the underlying disease. Identification of risk factors for progression can provide insight into the mechanisms of progressive loss of kidney function as well as identification of patients at higher risk for adverse outcomes. One of the questions posed by the Work Group was: What are the risk factors associated with a more rapid loss of kidney function?
Cardiovascular Disease
The 1998 Report of the NKF Task Force on Cardiovascular Disease in Chronic Renal Disease drew attention to cardiovascular disease as an outcome of chronic kidney disease.9 The Task Force recommended that patients with chronic kidney disease be considered in the “highest risk group” for subsequent cardiovascular disease (CVD) events. The excess risk of cardiovascular disease is due, in part, to a higher prevalence of conditions that are recognized as risk factors for cardiovascular disease in the general population (“traditional” CVD risk factors) and to hemodynamic and metabolic factors characteristic of chronic kidney disease (“CKD-related” CVD risk factors).
In addition, the Task Force emphasized the high mortality from cardiovascular disease. Cardiovascular disease is the leading cause of death in patients with kidney failure. After adjusting for age, gender, race, and diagnosis of diabetes, mortality from cardiovascular disease is far higher in patients with kidney failure compared to the general population. Among patients treated by dialysis, the risk ranges from 500-fold higher in individuals aged 25–35 to 5-fold higher in individuals aged >85 years (Fig 6).
Figure 6 |
|
Cardiovascular mortality in the general population (NCHS) and in ESRD treated by dialysis (USRDS). CVD mortality defined by death due to arrhythmias, cardiomyopathy, cardiac arrest, myocardial infarction, atherosclerotic heart disease, and pulmonary edema in the general population (data from NCHS multiple cause mortality data files, ICD-9 codes 402, 404, 410-414, and 425-429, 1993) compared to ESRD treated by dialysis (data from USRDS special data request HCFA form 2746, field numbers 23, 26–29, and 31, 1994–1996). Reprinted with permission9. |
|
Excess mortality also appeared higher in kidney transplant recipients, despite the preferential selection of patients without cardiovascular disease for transplantation.
One of the questions posed by the Work Group was: Is chronic kidney disease a risk factor for the development of cardiovascular disease? Because of the well-known association of cardiovascular disease and diabetes, it seemed reasonable that the analysis should distinguish patients with diabetes from other causes of chronic kidney disease. Among patients with diabetes, the Work Group summarized information related to the association of chronic kidney disease and diabetic complications. Among patients with other causes of kidney disease, the Work Group summarized information related to the association of chronic kidney disease and cardiovascular disease.
Decreased GFR is associated with complications in virtually all organ systems. These complications are manifested first by high blood pressure and abnormalities in laboratory tests and then by symptoms and abnormalities in physical examination. In general, the severity of complications worsens as level of GFR declines, although the actual levels of GFR where the complications first appear and then worsen vary depending on the complication. Among the most important complications are high blood pressure, anemia, malnutrition, bone disease, neuropathy, and decreased overall functioning and well-being. At very low levels of GFR, these complications are common and collectively known as “uremia” or the “uremic syndrome.” The pathogenesis of these complications varies among organ systems and is often complex. In many cases, early treatment can prevent or ameliorate complications.
Since signs and symptoms of kidney failure appear and increase in severity as GFR declines, it should be possible to identify levels of GFR that are associated with the appearance of particular signs and symptoms. One of the questions posed by the Work Group was: What is the level of GFR at the onset of high blood pressure, anemia, malnutrition, bone disease, neuropathy, and decreased overall functioning and well-being?
Dialysis and transplantation are effective, although not optimal, therapies for kidney failure. The aging of the population and the rising prevalence of diseases causing chronic kidney disease, such as hypertension and diabetes, suggest that kidney failure will be a growing public health problem in the future and that dialysis and transplantation will become more widely used in the United States and around the world. These therapies require intensive resources; therefore, measures to increase the efficiency of these treatments will be necessary. It will be necessary to improve the preparation of patients for kidney replacement therapy, as well as to improve the efficacy of dialysis and transplantation.
Preparation for Kidney Replacement Therapy
Much of the morbidity of kidney failure is due to complications that arise during the stage of decreased GFR. Many studies have shown a relationship between severity of complications before kidney replacement therapy and outcomes15. Possibly, improved treatment during the stage of decreased GFR would lead to improved outcomes of kidney replacement therapy.
In addition, the onset of kidney failure is usually associated with severe psychosocial stress. Stress derives from the fear of complications, from treatment, from limitations of functioning and well being, and from reduced life expectancy. A team approach to the management of patients is usually required, including physicians, nurses, dietitians, social workers, pharmacists, and physical, occupational, and vocational rehabilitation professionals as well as patients’ families. Patient education must begin far in advance in order to prepare patients to cope with their illness and the demands of their treatment as well as possible. Clinical practice guidelines are being developed by the Renal Physicians Association to address preparation for kidney replacement therapy.
Dialysis and Transplantation
The past decade has seen dramatic improvements in dialysis and transplantation. Advances in basic science and technology are needed to pave the way for continuing improvement. Each advance will require careful clinical study to assess its efficacy, effectiveness, and efficiency. As discussed earlier, NKF-DOQI clinical practice guidelines were restricted primarily to the care of patients with kidney failure treated by dialysis. The original DOQI guidelines have now been updated and published under the KDOQI banner16. New guidelines are under development by the NKF and other organizations to address other aspects of dialysis care and the care of patients treated by kidney transplantation.
Finally, the Work Group attempted to integrate the classifications of stages, types (diagnosis), and clinical presentations of chronic kidney disease presented in this guideline. The results provide a simplified approach to common clinical problems in chronic kidney disease, including screening, differential diagnosis, utility of proteinuria in diagnosis and treatment, estimating and slowing progression, cardiovascular disease risk assessment and reduction, clinical evaluation of adults with decreased GFR, and decreased GFR and chronic kidney disease in the elderly.