Figure 25
Anemia work-up for patients with chronic kidney disease. Modified and reproduced with permission.265,266
GUIDELINE 8. ASSOCIATION OF LEVEL OF GFR WITH ANEMIA
Anemia usually develops during the course of chronic kidney disease and may be associated with adverse outcomes.
- Patients with GFR <60 mL/min/1.73 m2 should be evaluated for anemia. The evaluation should include measurement of hemoglobin level.
- Anemia in chronic kidney disease should be evaluated and treated—see KDOQI Clinical Practice Guidelines for Anemia of Chronic Kidney Disease, Guidelines 1 through 4, as shown in Fig 25.
Figure 25 |
|
Anemia work-up for patients with chronic kidney disease. Modified and reproduced with permission.265,266 |
|
It is well established that anemia develops in the course of chronic kidney disease and is nearly universal in patients with kidney failure.264 The development of effective therapeutic options, such as erythropoietin therapy, has provided for the effective treatment of anemia. An earlier KDOQI clinical practice guideline is devoted to this topic265,266; however, that guideline focused primarily on patients treated by dialysis. This guideline addresses anemia in the earlier stages of chronic kidney disease.
Importantly, past guidelines have relied on serum creatinine levels >2 mg/dL as the criterion to test for the presence of anemia. The Work Group recommends that the KDOQI Anemia guideline be updated to in corporate estimated GFR <60 mL/min/1.73 m2 to trigger the ascertainment of anemia, rather than the previously cited serum creatinine levels (Fig 25).
Definition of Anemia
Measures used to assess anemia and its causes include hemoglobin, hematocrit, and iron stores (as measured directly by bone marrow biopsy, or indirectly as measured by serum ferritin, transferrin saturation levels, and percentage of hypochromic red blood cells or reticulocytes). Erythropoietin levels are less useful as a measure of anemia in chronic kidney disease, since it is now well established that they are often not appropriately elevated despite low hemoglobin levels.267-271
Measurement of hemoglobin, rather than hematocrit, is the preferred method for assessing anemia. Unfortunately, this issue has been confused due to the use of hematocrit in a number of studies. Hematocrit is a derived value, affected by plasma water, and thus subject to imprecision as a direct measure of erythropoiesis. Measurement of hemoglobin gives an absolute value and, unlike hematocrit, is not affected greatly by shifts in plasma water, as may occur with diuretics or with dialysis therapy. Hemoglobin levels are directly affected by lack of erythropoietin production from the kidney and thus serve as a more precise measurement of erythropoiesis.
While decreased hemoglobin often accompanies chronic kidney disease, there is no quantitative definition of anemia in chronic kidney disease, since "acceptable" (normal) hemoglobin levels have not been defined for patients with kidney disease. Instead, anemia is defined according to physiological norms. All patients with chronic kidney disease who have hemoglobin levels lower than physiological norms are considered anemic.
The definition of anemia in chronic kidney disease is further complicated by gender differences in hemoglobin levels. In the normal population, hemoglobin levels vary between genders and also as a function of menopausal status. The World Health Organization defines anemia to be that level of hemoglobin and gender-determined normal ranges without reference to age or menopausal status.272 Thus, for males, anemia is defined as hemoglobin level <13.0 g/dL, while in women, anemia is defined as hemoglobin level <12.0 g/dL. The WHO is in the process of updating these definitions to expand and refine them with specific levels in pregnant women and children of different ages. In most studies of anemia related to the level of kidney function, these issues have not been taken into account.
The operational definition of anemia in patients with kidney disease has also been influenced by health policy. In the past, national reimbursements (such as Medicare and Medicaid in the United States) have required the attainment of specific levels of hemoglobin or hematocrit, leading investigators and clinicians to define anemia relative to those regulatory levels. As stated in the European Best Practice Guidelines for the Management of Anaemia,273 it is important to define anemia relative to physiological norms rather than payment rules.
Some studies have arbitrarily defined the "anemia" of kidney disease as a hemoglobin level below some discretionary level (eg, 10 g/dL) that is well below the normative values in the general population. The low hemoglobin level that is often seen in chronic kidney disease should not lead to the acceptance of lower than normal hemoglobin levels as appropriate in patients with chronic kidney disease.
Strength of Evidence
Anemia develops during the course of chronic kidney disease (R). Lower hemoglobin may result from the loss of erythropoietin synthesis in the kidneys and/or the presence of inhibitors of erythropoiesis. Numerous articles document the association of anemia with kidney failure and describe its various causes.267,268,274-276 The severity of anemia in chronic kidney disease is related to the duration and extent of kidney failure. The lowest hemoglobin levels are found in anephric patients and those who commence dialysis at very severely decreased levels of kidney function.271,277,278
Anemia is associated with worse outcomes in chronic kidney disease (R). As yet it is undetermined whether the presence of anemia in chronic kidney disease directly worsens prognosis or whether it is a marker for the severity of other illnesses. Definitive studies have not been concluded. The available evidence, consisting of large database analysis and population studies, clearly show that low hemoglobin levels are associated with higher rates of hospitalizations, cardiovascular disease, cognitive impairment, and other adverse patient outcomes, including mortality.279-284
Erythropoietin deficiency is the primary cause of anemia in chronic kidney disease (R). Anemia in patients with chronic kidney disease is due to a number of factors, the most common of which is abnormally low erythropoietin levels. Other causes include: functional or absolute iron deficiency, blood loss (either occult or overt), the presence of uremic inhibitors (eg, parathyroid hormone, spermine, etc), reduced half life of circulating blood cells, deficiencies of folate or Vitamin B12, or some combination of these with a deficiency of erythropoietin.267-269,274,275 Patients with kidney disease may have concurrent underlying hematological problems such as thalassemia minor, sickle cell disease, or acquired diseases such as myelofibrosis or aplastic anemia.
The causative role of erythropoietin deficiency in anemia of chronic kidney disease includes: (1) anemia is responsive to treatment with erythropoietin in all stages of chronic kidney disease; and (2) in patients with chronic kidney disease, circulating levels of erythropoietin are not sufficient to maintain hemoglobin within the normal range. North American (United States and Canada) and European studies have demonstrated these points.270,271,282,285-287
Onset and severity of anemia are related to the level of GFR; below a GFR of approximately 60 mL/min/1.73 m2, there is a higher prevalence of anemia (Tables 76 and 77 and Figs 26, 27, 28, and 29) (C, S).
Figure 26 |
|
Blood hemoglobin percentiles by GFR adjusted to age 60 (NHANES III). Median and 5th and 95th percentiles of hemoglobin among adult participants age 20 years and older in NHANES III, 1988 to 1994. Values are adjusted to age 60 years using a polynomial quantile regression. The estimated GFR for each individual data point is shown with a plus sign (+) near the abscissa. 95% confidence intervals at selected levels of estimated GFR are demarcated with triangles, squares, and circles. |
|
Figure 27 |
|
Adjusted prevalence in adults of low hemoglobin by GFR (NHANES III). Predicted prevalence of hemoglobin <11 and <13 g/dL among adult participants age 20 years and older in NHANES III, 1988 to 1994. Values are adjusted to age 60 years using a polynomial regression. 95% confidence intervals are shown at selected levels of estimated GFR. |
|
Figure 28 |
|
Hemoglobin percentiles by GFR. These data are based on the results of 446 patients enrolled in the Canadian Multicentre Longitudinal Cohort study of patients with chronic kidney disease. All patients were referred to nephrologists between 1994 and 1997. No patient was receiving erythropoietin therapy at the time of enrollment, and no patient had an AV fistula. Adapted and reprinted with permission.288 |
|
Figure 29 |
|
Prevalence of low hemoglobin by GFR category. These data are based on the results of 446 patients enrolled in the Canadian Multicentre Longitudinal Cohort study of patients with chronic kidney disease. All patients were referred to nephrologists between 1994 and 1997. No patient was receiving erythropoiten therapy at the time of enrollment, and no patient had an AV fistula. Adapted and reprinted with permission.288 |
|
Studies reviewed for the purposes of this guideline include those of patients with chronic kidney disease prior to dialysis, those with kidney transplants, and those on dialysis.
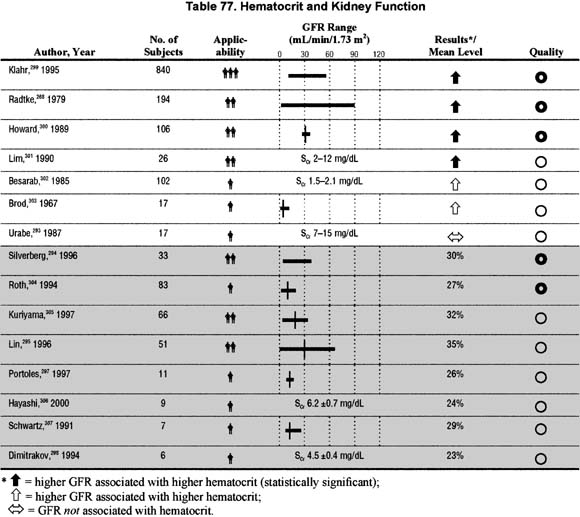
The reviewed literature spans almost 30 years of investigation and describes the clinical findings of researchers as they explore the relationships between hemoglobin and kidney function (Tables 76 and 77). The majority of available data have been derived from studies of small sample size, most of which are cross-sectional studies or baseline data from clinical trials of variable size and robustness. These studies are predominantly of only moderate or modest quality from a methodological standpoint. The consistency of the information they provided does, however, indicate a trend toward lower hemoglobin levels at lower levels of GFR and a variability in hemoglobin levels across GFR levels.
In 12 of the 22 studies reviewed, there was an association between the level of hemoglobin or hematocrit and the selected measure of kidney function. Data obtained from the NHANES III analysis (Fig 26) demonstrates an association between hemoglobin and level of GFR at GFR levels <90 mL/min/1.73 m2. While the increase in prevalence of anemia is most notable in the population studied at GFR levels <60 mL/min/1.73 m2, anemia can be present in patients with higher GFR levels. Due to the sparcity of data points at values <30 mL/min/1.73 m2 in the NHANES III database, the Canadian Multicentre Study288 was utilized to demonstrate trends in a large cohort of patients prior to dialysis (Fig 28). Note in Fig 29 the increase in prevalence of anemia at lower levels of GFR, but the existence of up to 20% of patients with anemia at higher, though still abnormal levels of GFR (30 to 44 mL/min/1.73 m2). Thus, the NHANES III data are consistent with data derived from populations with kidney disease and lower GFR288 (Figs 28 and 29).
Published studies cited in Tables 76 and 77 demonstrate a variability in the levels of hemoglobin or hematocrit at each level of kidney function, whether assessed by serum creatinine concentration, creatinine clearance, or GFR. These observations underscore the need to measure hemoglobin levels in every individual with GFR <60 mL/min/1.73 m2 and to individualize the assessment of anemia. The population-based trend toward lower hemoglobin levels as GFR falls does not yield a predictable progression that can be applied to individual patients. Thus, anemia should be considered in some patients with chronic kidney disease and GFR >60 mL/min/1.73 m2.
Erythropoietin levels are not consistently associated with the level of GFR (Table 78) (C).

Erythropoietin levels in patients with chronic kidney disease have not been well characterized in studies to date and do not appear to be directly related to level of kidney function. The majority of studies have been performed in patients already receiving dialysis, though some studies describe the relationship of erythropoietin levels to GFR in diabetics and in patients not on dialysis.275,308,309
The consistent finding apparent from these studies is that, for any given level of kidney function and anemia, the erythropoietin levels are lower in individuals with kidney disease than in those with anemia but normal kidney function.
The interpretation of these findings is that patients with kidney disease, as compared to normal individuals, do not have an appropriate rise in the levels of erythropoieten in the presence of anemia; while levels may be higher than non-anemic chronic kidney disease patients, the rise in erythropoietin levels is not commensurate with that seen in patients with the same degree of anemia but without kidney disease. Table 77 shows the paucity of data in this area and the weakness of the association demonstrated by published studies between erythropoiten levels and level of kidney function.
Measures of iron stores, including ferritin and transferrin saturation, are not consistently associated with the level of GFR (Tables 79 and 80) (C).
Several measures of iron stores have been studied in patients with kidney disease. Most of these measures, unlike bone marrow biopsy, do not directly quantify the amount of iron available for use in erythrocyte synthesis, relying instead on indirect or surrogate measures. Ferritin levels in patients with reduced GFR may represent total body iron status, or they may simply be markers of inflammation. Given the "chronic inflammatory state" that may characterize chronic kidney disease, ferritin levels are not useful in measuring iron stores, nor in predicting the relation of hemoglobin to kidney function.
Transferrin saturation, in combination with serum iron and ferritin levels, may be helpful in diagnosing functional iron deficiency—just as low serum ferritin levels are helpful in diagnosing iron deficiency anemia.311,312 However, there is little correlation of iron measurements with stages of kidney disease.
This analysis is limited by a lack of data about the relationship of levels of hemoglobin and kidney function in a truly representative sample of patients with chronic kidney disease. Many of the published studies describe patients entered into clinical trials or seen by nephrologists. The reasons for these differences are incompletely studied but noted in conventional texts and review articles.277,313
Interestingly, specific subgroups of patients (such as those with polycystic kidney disease) may have erythropoietin synthesis that is better preserved than other subgroups (such as diabetics). In the subgroup of patients who have kidney transplants, there are multiple causes for anemia in addition to decreased kidney function. The use of immunosuppressive agents or other medications, or chronic inflammation due to transplant rejection, may further confound the assessment of the etiology of declining hemoglobin. However, it is clear that at given levels of compromised GFR, kidney transplant patients do demonstrate reduced levels of hemoglobin, consistent with findings in patients with native diseased kidneys, and with those who have impaired kidney function.310
Another limitation of the current analysis is the variety (and lack of precision) of methods by which kidney function was measured in studies that assessed hemoglobin in patients with chronic kidney disease. Methods used included: measured GFR (iothalamate or other methods), calculated GFR (using different equations), measured or calculated creatinine clearance (using different equations). It is therefore difficult to determine whether the variability in hemoglobin at levels of kidney function is due to variability in measurements of kidney function or to variability associated with chronic kidney disease itself. While true variability between patients is the more likely possibility, the magnitude of variability is unknown.
Available data permit the description of mean levels of hemoglobin (with wide standard deviations) at different levels of GFR and support the following recommendations. Physicians treating patients with chronic kidney disease should:
These recommendations are consistent with published KDOQI Clinical Practice Guidelines on Anemia of Chronic Kidney Disease.266 While there are no "normal"/expected values of hemoglobin at any specific level of GFR, available data suggest that individual patients do trend toward a fall in hemoglobin as kidney function declines. The characterization of severity of anemia for any individual with chronic kidney disease should be made in light of changes in hemoglobin from previous levels. The decline in hemoglobin is most likely associated with a reduction in erythropoietin effectiveness or production, which accompanies the decline in GFR.
Treatment and assessment recommendations are beyond the scope of this guideline but are provided in the KDOQI Clinical Practice Guidelines on Anemia of Chronic Kidney Disease266 and the European Best Practice Guidelines for the Management of Anaemia in Patients with Chronic Renal Failure.273
Clearly, more information is needed on hemoglobin levels in chronic kidney disease—especially in patients in the early stages of kidney disease and as kidney function declines. Future studies should include:
{kind=link}