7.1 Treatment of catheter dysfunction:
Catheter dysfunction should be treated when a dialyzer blood flow of 300 mL/min is not being attained in a catheter previously able to deliver greater than 350 mL/min at a prepump pressure of –250 torr.
- 7.1.1 A dysfunctional catheter (blood flow < 300 mL/min) for 2 consecutive treatments should be treated in the HD unit by using an intraluminal interdialytic thrombolytic lock protocol between 2 dialysis treatments (ie, 35 to 69 hours).
7.2 Radiological evaluation:
Any dysfunction that cannot be managed in the dialysis unit should be sent for radiographic study to diagnose dysfunction and document the condition of the vessel.
- 7.2.1 Catheter imaging with contrast infusion can identify other correctable problems (eg, residual lumen thrombus, external fibrin catheter sheath, malpositioned catheter tip). Appropriate interventions may follow, such as:
- 7.2.1.1 Repositioning of the catheter.
- 7.2.1.2 Angioplasty of a vessel.
- 7.2.1.3 Replacement of a malpositioned catheter over guide wire.
- 7.2.1.4 Higher-dose lytic infusion for occlusive thrombus (eg, right atrial) or fibrin sheath
7.3 Choice of thrombolytic and use of other modalities:
- 7.3.1 A special brush is used to remove thrombus from the lumens of a conventional catheter by using a protocol specific to this procedure.
7.4 Treatment of infection:
- 7.4.1 Catheter exit-site infections, in the absence of a tunnel infection, should be treated with topical and/or oral antibiotics, ensuring proper local exit-site care. In general, it should not be necessary to remove the catheter.
- 7.4.2 If a patient with bacteremia is afebrile within 48 hours and is clinically stable, catheter salvage might be considered by using an interdialytic antibiotic lock solution and 3 weeks of parenteral antibiotics in appropriate situations. A follow-up blood culture 1 week after completion of the course of antibiotics should be performed. (see Table 24)
- 7.4.3 Antibiotic lock with antibiotic to which the organism is sensitive is indicated when follow-up cultures indicate reinfection with the same organism in a patient with limited catheter sites.
- 7.4.4 Short-term catheters should be removed when infected. There is no conclusive evidence to support a rationale for scheduled replacement except for those in the femoral area.
Treatment of Catheter Dysfunction (CPR 7.1)
Locking with tPA maintains the conductance of a catheter better than locking with heparin.496 Alternatively, intracatheter lytic infusion (eg, UK, 20,000 U/lumen/h for 6 hours,600 or alteplase, 2.5 mg/lumen over 1 to 2 hours) during the dialysis can restore blood flow.601,602
Several studies evaluated the effect of tPA infusion in restoring patency to dysfunctional catheters. In general, infusion of 1 to 4 mg/lumen over 1 to 4 hours permits restoration of flow (>200 mL/min) sufficient to permit completion of a dialysis treatment,601-603 permitting control of serum potassium levels and fluid removal. Infusion may succeed when a simple timed dwell fails. The difference in efficacy may result from the amount of lytic that gets to the fibrin/thrombus in a limited time. With the dwell technique, only the lytic at the catheter tip is biochemically active; the amount that has not leaked immediately must slowly diffuse to the fibrin or thrombus at the tip or exterior to the catheter. Conversely, push or infusion techniques more rapidly deliver the lytic in the lumen to the area of need. However, there have been no head-to-head comparisons. There should be little fear to use tPA as a long lock dwell or as infusions of doses less than 10 mg. The half-life of tPA is on the order of minutes, and it is only active when bound to fibrin. At the doses and infusion rates used, there is virtually no risk for systemic thrombolytic effect.
Very few head-to-head comparisons have been made among the available lytics.525,604,605 Two studies showed an advantage of tPA over UK, but neither was randomized. In 1 of the studies, “the push” protocol was used as opposed to the “passive dwell.”525 The choice of agent to be used is governed by many factors, including availability, convenience, cost, and comparative efficacy.
Unfortunately, when the fibrin deposition/thrombus formation process is allowed to advance to a severe degree, the occlusive process recurs and repeated doses of lytic must be administered496,516,517,523 at a median intertreatment interval of only 5 to 7 additional dialysis sessions.516 This is believed to result from the presence of a fibrin sheath that, at times, is so extensive as to occlude the SVC.606
Endoluminal brushing, although not used widely in the United States, can remove clots effectively and also provides material for culture to rule out or confirm infection.528
Radiological Evaluation (CPR 7.2)
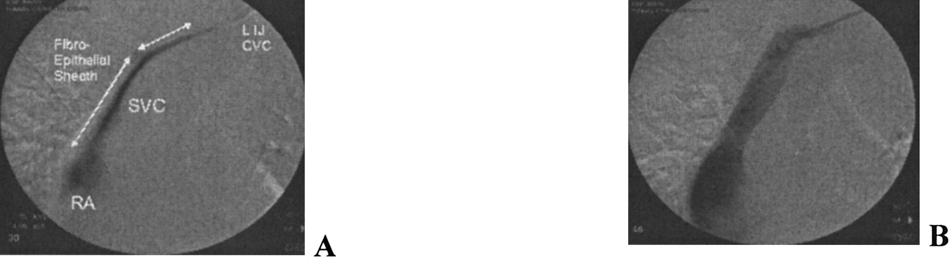
A fibrin sheath can only be diagnosed by performing a contrast study and requires partial pull back of the catheter. A representative example is shown in Fig 10.
Fig 10. Fibrin sheath (A) prior to therapy; (B) after treatment with PTA. Abbreviations: LIJ, Left internal jugular; RA, Right atrium; SVC, Superior Vena Cava. (Courtesy of Dr A. Asim).
A fibrin sheath can be treated in 1 of several ways: fibrin sheath stripping, guide wire catheter exchange, and lytic infusion.156,157,579,607-609 Studies have shown the success of tPA infusion,607,608 as well as stripping of the catheter.156,609 No difference in outcome was found between percutaneous stripping and UK infusion.530 See Table 24 in CPG 7.6 for additional information.
There have been no comparisons of sheath disruption with an angioplasty balloon compared with the other 2 techniques. It is intermediate in complexity. Until such studies are done, the Work Group's preferred intervention for a fibrin sheath is removal of the catheter over a guide wire, disruption of the sheath with a balloon, and placement of a new catheter (catheter exchange).531
Catheter Maintenance (CPR 7.3)
Increasing focus should be placed on prevention or control of growth of the fibrin sheath through periodic high-dose lytic infusion600 triggered by a progressive decrease in achievable BFR. Also, some centers are using weekly instillation of tPA or UK to maintain flow characteristics of long-term catheters.496,531 There is sufficient evidence of effectiveness for the Work Group to recommend these approaches for long-term catheter management with the proviso that this is an area for future research to optimize the best regimens that are cost-effective.