GUIDELINE 4. ESTIMATION OF GFR
Estimates of GFR are the best overall indices of the level of kidney function.
The level of GFR should be estimated from prediction equations that take into account the serum creatinine concentration and some or all of the following variables: age, gender, race, and body size. The following equations provide useful estimates of GFR:
- In adults, the MDRD Study and Cockcroft-Gault equations
- In children, the Schwartz and Counahan-Barratt equations.
- The serum creatinine concentration alone should not be used to assess the level of kidney function.
- Clinical laboratories should report an estimate of GFR using a prediction equation, in addition to reporting the serum creatinine measurement.
- Autoanalyzer manufacturers and clinical laboratories should calibrate serum creatinine assays using an international standard.
Measurement of creatinine clearance using timed (for example, 24-hour) urine collections does not improve the estimate of GFR over that provided by prediction equations. A 24-hour urine sample provides useful information for:
- Estimation of GFR in individuals with exceptional dietary intake (vegetarian diet, creatine supplements) or muscle mass (amputation, malnutrition, muscle wasting);
- Assessment of diet and nutritional status;
- Need to start dialysis.
Glomerular filtration rate (GFR) provides an excellent measure of the filtering capacity of the kidneys. A low or decreasing GFR is a good index of chronic kidney disease. Since the total kidney GFR is equal to the sum of the filtration rates in each of the functioning nephrons, the total GFR can be used as an index of functioning renal mass.111 A decrease in GFR precedes kidney failure in all forms of progressive kidney disease. Monitoring changes in GFR can delineate progression of kidney disease. The level of GFR is a strong predictor of the time to onset of kidney failure as well as the risk of complications of chronic kidney disease. Additionally, estimation of GFR in clinical practice allows proper dosing of drugs excreted by glomerular filtration to avoid potential drug toxicity.
Glomerular filtration rate cannot be measured directly. If a substance in stable concentration in the plasma is physiologically inert, freely filtered at the glomerulus, and neither secreted, reabsorbed, synthesized, nor metabolized by the kidney, the amount of that substance filtered at the glomerulus is equal to the amount excreted in the urine. The fructose polysaccharide inulin has each of the above properties and has long been considered an ideal substance to estimate GFR. The amount of inulin filtered at the glomerulus equals the GFR multiplied by the plasma inulin concentration: GFR × Pin. The amount of excreted inulin equals the urine inulin concentration (Uin) multiplied by the urine flow rate (V, volume excreted per unit time).
Since filtered inulin = excreted inulin:
(1) GFR×Pin=Uin×V
(2)![]()
The term (Uin × V)/Pin is defined as the clearance of inulin and is an accurate estimate of GFR. The inulin clearance, in mL/min, refers to that volume of plasma per unit time that is cleared of inulin by renal excretion.
Criterion Standard
Inulin clearance is widely regarded as the gold standard for measuring glomerular filtration rate. Inulin clearance measurements in healthy, hydrated young adults (adjusted to a standard body surface area of 1.73 m2) have mean values of 127 mL/min/1.73 m2 in men and 118 mL/min/1.73 m2 in women with a standard deviation of approximately 20 mL/min/1.73 m2.67 Among adults, numerous studies suggest that glomerular filtration rate is lower at older ages. After age 20 to 30 years, GFR decreases by approximately 1.0 mL/min/1.73 m2 per year with substantial inter-individual variation even among “healthy” individuals.112,113 Whether this average decline with aging is optimal in terms of predicting the risk of complications of decreased kidney function and mortality is unknown.
Glomerular filtration rate in the infant differs quantitatively from that in older children and adults. During infancy and through the first 12 to 18 months of life, GFR increases with maturation69-71 (see Table 23, Guideline 1). Inulin clearance is also the gold standard to measure GFR in children, but is particularly difficult in the neonate because of the lower GFR of neonates and their relatively larger extracellular fluid compartment. These factors extend the study time necessary for techniques relying on equilibration of the marker substance and monitoring of its plasma disappearance rate. Additionally, accurate assessment of the urine flow rate requires bladder catheterization in infants and young children.
Rationale for Alternative Measures
The classic method of inulin clearance requires an intravenous infusion and timed urine collections over a period of several hours making it costly and cumbersome. As a result a number of alternative measures for estimating GFR have been devised. The urinary clearance of exogenous radioactive markers (125I-iothalamate and 99mTc-DTPA) provide excellent measures of GFR114 but are not readily available. Plasma clearance of exogenous substances including iohexol and 51Cr-EDTA has been used as well but require estimates of body size, which decreases their precision. Capillary electrophoresis allows for measurement of non-radiolabeled iothalamate in blood and urine with promising results.115 Serum cystatin C has been used to estimate GFR but data are conflicting as to whether it provides a sufficient improvement to warrant widespread clinical use.116 The most widely used measures of GFR in clinical practice are based on the 24-hour creatinine clearance or serum creatinine concentration. As discussed below, each of these measurements is associated with serious limitations.
Equations to predict GFR and creatinine clearance from serum creatinine have been tested in a large number of studies whose results are reviewed. Use of relevant equations in children and adults has been shown to give more valid estimates of GFR than serum creatinine alone. Additionally, for the health care provider, it may be easier to recognize clinically important changes in kidney function when dealing with large numbers estimating a physiologically relevant parameter (GFR) rather than small numbers (serum creatinine) which are inversely related to the relevant parameter.
Accuracy of an Equation in Estimating GFR Combines Its Bias and Precision
In choosing a prediction equation to estimate GFR, one should consider both the bias and precision of the equation-generated estimates. Bias expresses the systematic deviation from the gold standard measure of GFR. A prediction equation that consistently overestimates or underestimates the gold standard measure of GFR yields a biased estimate.
An equally important measure of the usefulness of a prediction equation is a measure of its precision. Precision expresses the variability (or dispersion) of prediction equation estimates around the gold standard GFR measure.
Accuracy combines precision and bias. A useful measure of accuracy is a description of percentiles of the distribution of the differences between estimated and measured GFR. In other words, if 99% of the time a prediction equation yields an estimate within 10% of the measured GFR, it would be a very accurate and useful clinical tool. Achieving a high level of accuracy requires both low bias and high precision. Description of the percent of estimates falling within 30% and 50% above or below the measured GFR is a useful measure of accuracy.
Importance of Sample Size
Many of the studies reviewed were small. Since estimates of accuracy from smaller studies can be unreliable, studies presented have at least 100 adults or 50 children. Several large validation studies evaluating the newly developed MDRD Study equation were conducted recently and were only available in abstract form. In order to capture these valuable data the authors were contacted and asked to analyze their data and provide estimates of accuracy for this review. Additional details regarding the evaluation of prediction equations to estimate GFR are reviewed in Part 10, Appendix 3.
Strength of Evidence
Serum creatinine alone is not an accurate index of the level of GFR (R). The use of the serum level of creatinine as an index of GFR rests on three important assumptions: (1) creatinine is an ideal filtration marker whose clearance approximates GFR; (2) creatinine excretion rate is constant among individuals and over time; and (3) measurement of serum creatinine is accurate and reproducible across clinical laboratories. Although the serum creatinine concentration can provide a rough index of the level of GFR, none of these assumptions is strictly true, and numerous factors can lead to errors in estimation of the level of GFR from the serum creatinine concentration alone.
Creatinine excretion by the kidney. Creatinine is freely filtered by the glomerulus, but is also secreted by the proximal tubule. Hence, the amount of creatinine excreted in the urine is the composite of both the filtered and secreted creatinine and can be represented by the following equation:
(3) UCr×V=GFR×PCr+TSCr
where TSCr is the rate of tubular creatinine secretion. Dividing by PCr:
(4) CCr=GFR+CTSCr
where CTSCr is the clearance of creatinine due to tubular secretion. Thus, creatinine clearance systematically overestimates GFR. This overestimation is approximately 10% to 40% in normal individuals, but is greater and more unpredictable in patients with chronic kidney disease (Fig 12).
Figure 12 |
|
Relationship of creatinine clearance and serum creatinine with GFR (inulin clearance) in patients with glomerular disease. Vertical dashed lines correspond to the lower limit of normal for inulin clearance in the authors’ laboratory (82 mL/min/1.73 m2). The horizontal dashed line in the left panel (A) corresponds to the lower limit for creatinine clearance (77 mL/min/1.73 m2); and the horizontal dashed line in the right panel (B) corresponds to the upper limit for the serum creatinine concentration (1.4 mg/dL) in the authors’ laboratory. The shaded areas included values for patients in whom GFR is reduced, but creatinine clearance and serum creatinine concentration remain normal. Data from Shemesh et al.117 Reprinted with permission.118 |
|
Factors other than the level of GFR can also influence creatinine secretion. Creatinine secretion is inhibited by some common medications, for example, cimetidine and trimethoprim.
In addition, measurement of creatinine clearance is not easy. Urinary clearance measurements require timed urine collections, which are difficult to obtain and often involve errors in collection. Furthermore, day-to-day variation in creatinine excretion exists, making estimation of GFR, even from a valid 24-hour urine collection, imprecise.
Creatinine metabolism. The urinary creatinine excretion represents the difference between creatinine generation in the body (GCr) and extra-renal creatinine elimination (ECr):
(5) UCr×V=GCr-ECr
Substituting into equation 3 and re-arranging for PCr yields the following:
(6) ![]()
It can therefore be inferred that the relationship between serum creatinine and GFR is affected by the generation and extra-renal excretion of creatinine, as well as the filtration and secretion of creatinine by the kidney.
Creatinine is mainly derived from the metabolism of creatine in muscle, and its generation is proportional to the total muscle mass. As a result, mean creatinine generation is higher in men than in women, in younger than in older individuals, and in blacks than in whites. This leads to differences in serum creatinine concentration according to age, gender, and race, even after adjusting for GFR. Muscle wasting is also associated with reduced creatinine generation resulting in lower serum creatinine concentration than expected for the level of GFR in malnourished patients with chronic kidney disease. Creatinine generation is also affected by meat intake to a certain extent, because the process of cooking meat converts a variable portion of creatine to creatinine. Therefore, serum creatinine is lower than expected for the level of GFR in patients following a low protein diet.
Though extra-renal creatinine excretion is minimal in people with normal kidney function, it is increased in patients with chronic kidney disease due to the degradation of creatinine by bacterial overgrowth in the small bowel. As much as two-thirds of total daily creatinine excretion can occur by extra-renal creatinine elimination in patients with severely reduced kidney function.
As a consequence of all these factors, urinary creatinine excretion is lower in chronic kidney disease, leading to systematic overestimation of GFR from serum creatinine. Figure 12B shows that serum creatinine can remain less than 2.0 mg/dL despite reduction in GFR to as low as 15 to 20 mL/min/1.73 m2. Thus, an elevated serum creatinine is an insensitive index of decreased GFR. Only 60% of patients with decreased GFR had increased serum creatinine. Stated otherwise, 40% of individuals with decreased GFR had a serum creatinine level within the normal range for the laboratory.
Creatinine measurement. In young adults, the normal level for serum creatinine concentration is approximately 1.0 mg/dL. The traditional assay for measurement of creatinine is the alkaline picrate method, which detects non-creatinine chromogens in serum (approximately 0.2 mg/dL), as well as creatinine. Urine does not contain non-creatinine chromogens, nor are these compounds retained in chronic kidney disease. Thus, historically, measured creatinine clearance has systematically underestimated true creatinine clearance. By coincidence, the difference between measured and true creatinine clearance is similar in magnitude to the clearance of creatinine due to tubular secretion. Hence, measured creatinine clearance has historically approximated the level of GFR.
Modern autoanalyzers use serum creatinine assays with less interference by non-creatinine chromogens (for example, kinetic alkaline picrate or enzymatic methods, such as the imidohydrolase method). Consequently, normal levels of serum creatinine are now lower, resulting in higher values for measured creatinine clearance and overestimation of GFR. In order to minimize this overestimation of GFR, autoanalyzer manufacturers and clinical laboratories may calibrate the instruments to report higher serum creatinine values. This calibration is not standardized, leading to variation within and across laboratories. Variation is proportionately greater at low serum creatinine values than at high values.
In addition to non-creatinine chromogens, other substances may also interfere with serum creatinine assays. These substances include ketones and some medications, which may lead to spurious elevation in serum creatinine concentration and underestimation of GFR.
In summary, serum creatinine is affected by the level of GFR and by factors independent of GFR, including age, gender, race, body size, diet, certain drugs, and laboratory analytical methods (Table 43).

Therefore, serum creatinine is not an accurate index of the level of kidney function, and the level of serum creatinine alone should not be used to assess the stage of chronic kidney disease.
Equations estimating GFR based on serum creatinine are more accurate and precise than estimates of GFR from measurement of serum creatinine alone (R, C). Many studies have documented that creatinine production varies substantially across sex, age, and ethnicity.113 Equations have the advantage of providing an estimate of GFR which empirically combines all of these average effects while allowing for the marked differences in creatinine production between individuals. Figures 13 and 14 show that equation-based estimates perform better than serum creatinine alone.
Figure 13 |
|
Estimates of GFR versus measured GFR among MDRD Study baseline cohort. GFR measured as urinary clearance of 125I-iothalamate and adjusted for body surface area in 1,628 patients. Estimates include (A) 100/SCr (R2 = 80.4%), (B) Cockcroft-Gault equation standardized for body surface area (R2 = 84.2%), and (C) MDRD Study equation 7 (R2 = 90.3%). R2 values indicate the percentage of variance of log GFR accounted for in the validation sample (n = 558) by equations derived from the development sample (n = 1,070). Reprinted with permission.17 |
|
Figure 14 |
|
Accuracy of different estimates of GFR in adults, expressed as the percent of estimates within 30% and 50% of the measured GFR in the MDRD Study validation sample (n = 558). Estimates denoted with [C] include a calibration correction of 0.69 for 100/serum creatinine, 0.84 for Cockcroft-Gault equation, and 0.81 for 24-hour creatinine clearance to show performance after bias is eliminated using a multiplicative correction factor. Analysis of MDRD Study17 data prepared by Tom Greene, PhD. |
|
A number of equations have been developed to predict GFR directly in adult patients (Table 44) and children (Table 45).
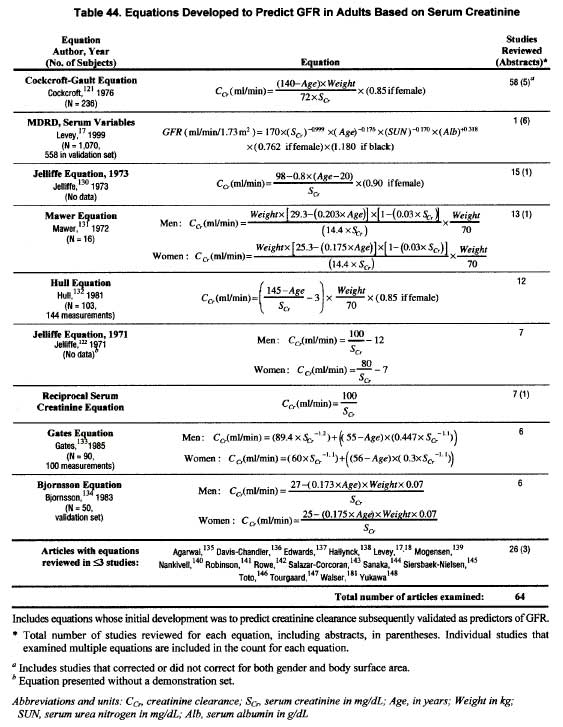
In addition to equations which directly predict GFR, the most frequently used equation for estimating GFR in adults is the Cockcroft-Gault equation which was developed for estimating creatinine clearance but has been tested widely in its prediction of GFR.120,121 Another equation developed in 1971 for estimation of creatinine clearance by Jelliffe has been used extensively.122
Several formulas for estimating GFR in children have been developed as well. The most widely studied of these are the Schwartz71,123-126 and Counahan-Barratt formulae.127-129 Both provide an estimate of GFR based on a constant multiplied by the child’s height divided by serum creatinine.
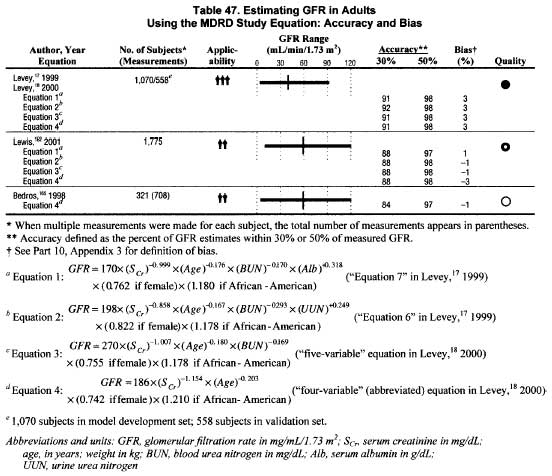
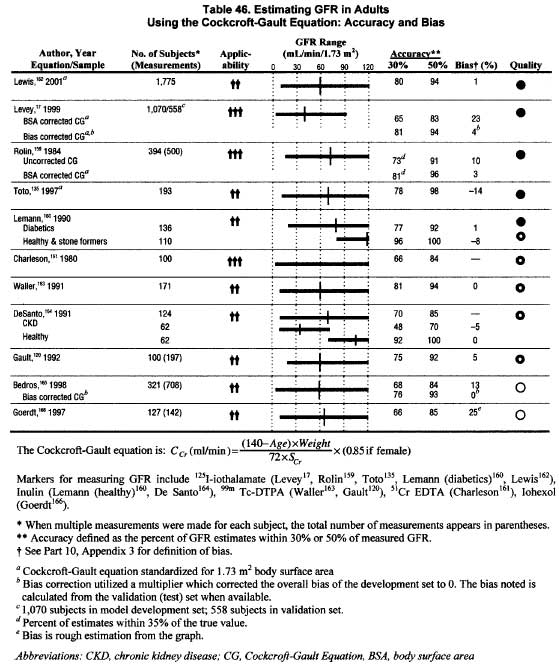
Many studies evaluate GFR prediction equations but several methodological aspects limit the ability to compare results across studies (C). A systematic review of the literature reveals that the number of references evaluating GFR prediction methods is vast (>100 references). Studies evaluating GFR prediction equations are listed in Table 46 (Cockcroft-Gault equation) and Table 47 (MDRD Study equation).
The presentation of validity data here is limited to four equations: the most widely used equations for estimating GFR in the adult (Cockcroft-Gault) and children (Schwartz and Counahan-Barratt) as well as the newly developed MDRD Study equations.
Techniques to measure creatinine, reference standards for GFR and the statistics used to estimate accuracy, bias, and precision vary widely in published reports. The most frequently used statistic is the correlation coefficient, which has little applicability and cannot be pooled across studies. While most reports specify the methods used to measure serum creatinine, only rarely is it known how closely the serum creatinine assay reflects the true creatinine level. This severely limits the ability to compare or combine reported results. (For details, see Part 10, Appendix 3.)
Among adults, the MDRD Study equation provides a clinically useful estimate of GFR (up to approximately 90 mL/min/1.73 m2) (S). The MDRD Study equation (Table 47) has the advantages of having been derived based on:
This equation provides estimates of GFR standardized for body surface area. The abbreviated version is easy to implement since it requires only serum creatinine, age, sex, and race. The calculations can be made using available web-based and downloadable medical calculators. The abbreviated MDRD Study equation has two equivalent forms (Table 48).
The results of studies reporting equations for estimating a standard measure of GFR with at least 100 adult participants and a plot of predicted versus measured GFR are summarized in Table 46 (Cockroft-Gault equation) and Table 47 (MDRD Study equation). The bias in estimating GFR using the Cockcroft-Gault equation varied markedly across studies (from -14% to +25%). The accuracy measures indicated the majority (median of 75%) of estimated GFRs were within 30% of the measured GFR, an accuracy considered sufficient for good clinical decision-making. The Cockroft-Gault equation does not include body size. Some studies have standardized the results for body surface area. Other studies have suggested using lean body mass rather than total weight, especially for obese individuals.
Table 47 shows similar data for several forms of the MDRD Study equation. Within the validation sample of the MDRD Study, the equation developed on an independent sample of 1,070 participants performed better than the Cockcroft-Gault equation (Fig 14). Over 90% of the estimates were within 30% of the measured GFR, with only 2% having an error of greater than 50%. The four different variants of the MDRD Study equation performed similarly using these criteria for accuracy in all of the available data. Thus, the abbreviated MDRD Study equation provides a rigorously developed equation for estimating GFR, which may allow for improved prediction of GFR. (See Part 10, Appendix 3.)
Table 49 shows serum creatinine values which can be used to identify individuals with an estimated GFR of 60 mL/min/1.73 m2 or less for adults of different ages, genders and ethnicities. All of the values are well below 2.0 mg/dL, which corresponds to an estimated GFR in the range of 25–51 mL/min/1.73 m2, depending on age, gender, and ethnicity. This equation may be superior to previous equations but the data at this point are quite limited. (See Part 10, Appendix 3) While this equation is difficult to memorize, it is available on the Internet (www.kdoqi.org) and can be readily programmed or imported into calculators and laboratory systems.
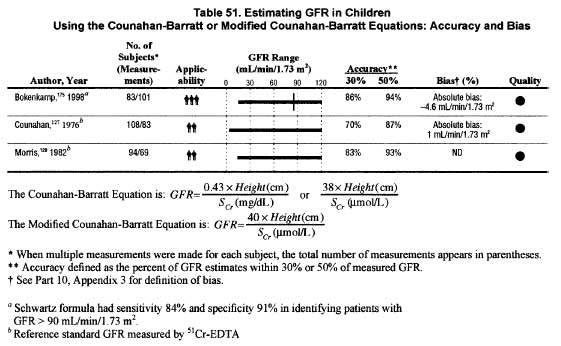
Among children, the Schwartz and Counahan-Barratt formulae provide clinically useful estimates of GFR (C). Several formulae for estimating GFR in children have been developed. Two of these, the Schwartz formula, and the Counahan-Barratt formulas utilize the proportionality between GFR and height/serum creatinine71,123-129 (Table 44). The difference between the constants cited in the Counahan-Barratt and the Schwartz formula has been attributed to the use of different assays to measure creatinine. The Counahan-Barratt formula was developed using a measure of “true” creatinine and GFR by 51Cr-EDTA plasma clearance, while the original Schwartz formula was developed using inulin clearance and creatinine measured by a modified Jaffe reaction, which may have overestimated true creatinine. Tables 49 and 50 show the results of studies reporting a standard GFR measure, at least 50 pediatric participants, and presenting a plot of predicted versus measured GFR, allowing assessment of the accuracy of the prediction equation in estimating GFR as outlined above.
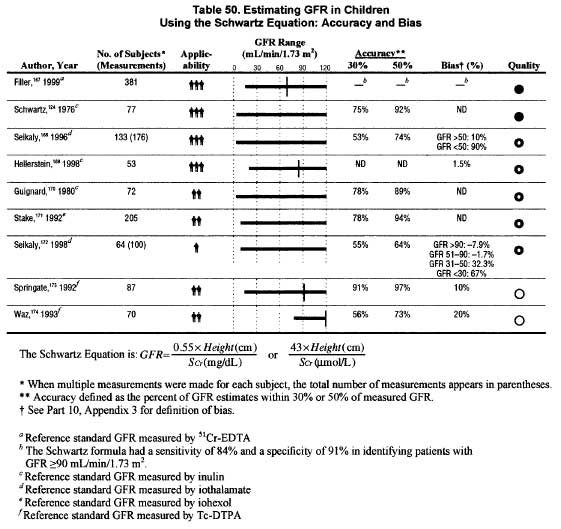
While a systematic review of the literature yielded over 40 references examining prediction equations to estimate GFR, only a handful used a gold standard measure of GFR and included more than 50 children (Tables 50 and 51).
For the Schwartz formula, most studies reported mean differences between estimated and measured GFR. These ranged from -0.4 to 10 mL/min/1.73 m2 with SD ranging from 2 to 20 mL/min/1.73 m2. The data suggest that the bias of the estimate of the Schwartz formula increases with decreasing GFR.168,172
Studies describing the accuracy of the estimate show that approximately 75% of Schwartz formula estimates of GFR are within 30% of the measured GFR by inulin clearance.124,170,171,176-180 Comparable studies of the Counahan-Barratt formula show 70% to 86% of Counahan-Barratt estimates fall within 30% of GFR measured by 51Cr-EDTA.
Although imprecise, the Schwartz and Counahan-Barratt formulae for estimating GFR in children are convenient and practical. Both use height in the estimate, as height is proportional to muscle mass. The constants used in the equations differ, likely related to the different assays to measure creatinine. For a 5-year-old child who is at median (50th percentile) height for age, the serum creatinine corresponding to a GFR of 60 mL/min/1.73 m2 is 1.0 mg/dL using the Schwartz formula and 0.8 mg/dL using the Counahan-Barratt formula. This example illustrates that use of both formulas can allow for estimation of kidney function, and even serum creatinine levels <1.0 mg/dL can be associated with substantially impaired kidney function in small children and adults who have low muscle mass or malnutrition.
Creatinine clearance over-estimates GFR; therefore, equations that accurately estimate creatinine clearance overestimate GFR when true creatinine is measured (R, S). The Cockcroft-Gault equation was developed to predict creatinine clearance rather than GFR. The equation was developed in a sample of men and a correction factor for women was proposed.121 The equation’s accuracy in predicting creatinine clearance from 24-hour urine has been evaluated in many publications (Table 46). Evaluation of these data is limited by the use of different assays and variable calibration within creatinine assays across laboratories and over time. Analogous statements apply to studies of the Schwartz formula in children.
The largest study that evaluated the Cockcroft-Gault equation in a single laboratory was the MDRD Study. The serum creatinine assay in this study was calibrated to approximate true creatinine. As a result, the Cockcroft-Gault equation over-estimated GFR by 23%.
Many of the studies evaluating the Schwartz formula in children have substituted creatinine clearance for GFR in assessing it bias and precision in different populations. The bias of Schwartz formula estimates compared to creatinine clearances is relatively small; however, the Schwartz formula has been shown to overestimate inulin clearance, particularly in children with low GFR.168,169,172 Although formulas that estimate creatinine clearance overestimate GFR, they provide an estimate that is accurate enough for most clinical purposes and represent a better alternative to assessing kidney function than serum creatinine alone.
Measuring 24-hour creatinine clearance to assess GFR is not more reliable than estimating GFR from a prediction equation (R). A 24-hour urine collection is useful for measurement of total excretion of nitrogen, electrolytes, and other substances. However, the use of 24-hour urine collection for the estimation of GFR has consistently been shown to be no more, and often less, reliable than serum creatinine based equations. A 1998 review181 found five of six studies that found serum creatinine based estimates of GFR to have a lower error than measured creatinine clearance in patients with kidney disease. In addition to collection errors, this is attributed to diurnal variation in GFR and day-to-day variation in creatinine excretion.
In children, several studies have compared the accuracy of prediction equations in estimating GFR with 24 hour or timed creatinine clearance studies.127,182-186 None of these studies demonstrated substantial improvement in estimating creatinine clearance using a 24-hour or timed urine collection over the use of either the Schwartz or Counahan-Barratt prediction equations. One relatively small study169 demonstrated a mean difference of 7.0 ± 17.8 mL/min/1.73 m2 between 24-hour creatinine clearance compared to GFR as measured by inulin clearance. Another documented 30% of 24-hour creatinine clearance studies yielded estimates of GFR more than 30% above or below GFR measured with iothalamate clearance.184
Important exceptions may be the estimation of GFR in individuals with variation in dietary intake (vegetarian diet, creatine supplements) or muscle mass (amputation, malnutrition, muscle wasting), since these factors are not specifically taken into account in prediction equations. In these situations, collection of a 24-hour urine sample for measurement of creatinine clearance, or measurement of clearance of an exogenous filtration marker, may provide better estimates of GFR than prediction equations.
Clinical laboratories should provide an estimate of GFR with the results of serum creatinine concentration (O). Laboratories that measure serum creatinine concentration should calculate GFR using an equation. Among adults, the MDRD Study equation may perform better than the Cockroft-Gault equation but the data are very limited. Among children, the Schwartz formula provides a clinically useful estimate of GFR. All four formulas reviewed provide a marked improvement over serum creatinine alone. Calculations by the laboratory, requiring only minimal clinical information, will facilitate the clinical interpretation of kidney function. The utilization of equations, some of which are complex, is much more efficient in the context of a centralized laboratory computer system than performed by individual physicians. Clinical laboratories will need to work with physicians and hospital or health center information system administrators to determine a number of practical issues: which prediction equation(s) to use; how to obtain the additional information required for the prediction equation; when to report estimated GFR (only when requested, or each time serum creatinine is measured); what additional information to include on the report (eg, normal values for age and gender, GFR levels for KDOQI CKD Stages). The laboratories should mind the importance of calibrating their serum creatinine to the same level as the laboratory in which the equation was developed. In this regard, development of international standards for calibration of serum creatinine assays will be important in allowing for the accurate diagnosis of Stage 2 chronic kidney disease.
Estimation of GFR or creatinine clearance from serum creatinine is critically dependent on calibration of the serum creatinine assay (R). There is substantial variation across laboratories in the calibration of serum creatinine, with systematic differences as large as 0.2 to 0.4 mg/dL not being uncommon. Such differences reflect a very large percentage of the serum creatinine in patients with a serum creatinine of 2.0 mg/dL or less. A 1987 review187 detailed 8 different existing methods to measure creatinine concentration. For patients with low muscle mass and serum creatinine ![]() 1.0 mg/dL, the more commonly used Jaffe and modified Jaffe reaction methods systematically overestimated creatinine by 20% to 80% compared to high performance liquid chromatography and dilution mass spectrometry measures which should approximate “true” creatinine. An analysis of College of American Pathologists survey data indicates that systematic differences in calibration of serum creatinine assays accounts for 85% of the difference between laboratories in serum creatinine. Much of the variation was within a method not just between methods. The laboratories surveyed averaged >13% bias in measurement of creatinine, larger than any other analyte examined, as well as substantial variation between laboratories in the bias. In comparison, reproducibility of the serum creatinine measures within a laboratory was much better (average coefficient of variation 8%).188 Standardization of the assay across laboratories is critical to the ability to diagnose and stage chronic kidney disease. Laboratories should inform clinicians which creatinine assay is used in their laboratory and how it compares to measures of “true” creatinine.
1.0 mg/dL, the more commonly used Jaffe and modified Jaffe reaction methods systematically overestimated creatinine by 20% to 80% compared to high performance liquid chromatography and dilution mass spectrometry measures which should approximate “true” creatinine. An analysis of College of American Pathologists survey data indicates that systematic differences in calibration of serum creatinine assays accounts for 85% of the difference between laboratories in serum creatinine. Much of the variation was within a method not just between methods. The laboratories surveyed averaged >13% bias in measurement of creatinine, larger than any other analyte examined, as well as substantial variation between laboratories in the bias. In comparison, reproducibility of the serum creatinine measures within a laboratory was much better (average coefficient of variation 8%).188 Standardization of the assay across laboratories is critical to the ability to diagnose and stage chronic kidney disease. Laboratories should inform clinicians which creatinine assay is used in their laboratory and how it compares to measures of “true” creatinine.
One reason for variation in the calibration of serum creatinine may have been a desire to provide a calculated 24-hour creatinine clearance that is closer to GFR. It is preferable to report estimates of appropriately calibrated true creatinine. The over-estimate of GFR by creatinine clearance can then be corrected explicitly using a correction factor. In the MDRD Study, this correction required multiplying the creatinine clearance by 0.81.17
A 24-hour urine sample should be collected to aid in the assessment of nutritional status and the need for kidney replacement therapy (O). The statements about the limited utility of 24-hour urine samples in estimating GFR do not apply to other uses of this urine collection. A 24 hour urine collection can be used to assess urea clearance, weekly Kt/Vurea, creatinine clearance, and dietary intake of protein, sodium, potassium, and phosphorus. For details on calculations of urea clearance, weekly Kt/Vurea, and dietary protein intake from 24 hour urine, see Part 10, Appendix 3. Guideline 1 reviews recommendations from DOQI guidelines regarding initiation of kidney replacement therapy. Guideline 9 reviews KDOQI guidelines on assessment of nutritional status.
In principle, accurate measurement of creatinine excretion in a timed urine collection at a single point in time could be used to improve the estimate of 24-hour excretion rates of various solutes from the ratio of solute-to-creatinine concentrations in untimed (“spot”) urine samples at later times. Alternatively, estimation of creatinine excretion from factors related to physiologic variables related to creatinine generation and extra-renal elimination (such as age, gender, race, body size, and GFR) could also be used to facilitate estimation of solute excretion rates from the ratio of solute-to-creatinine concentration in spot urine samples. Thus far, the accuracy of prediction equations for creatinine excretion have not been widely studied. Both methods may be limited, however, by variation in solute excretion rates during the day (as occurs with urea nitrogen in individuals with normal kidney function).
Steady State and Average Body Composition
Use of serum creatinine to estimate GFR relies on the individual being in steady state and the ability to estimate the average rate of production of creatinine. Therefore, estimates will be unreliable if the level of GFR is changing (such as acute kidney failure), if muscle mass is unusually high or low (such as athletes or malnourished individuals, respectively), or if dietary creatine intake is unusually high or low (such as individuals consuming creatine supplements or vegetarians, respectively). Methods proposed for estimating GFR in acute kidney failure189 were outside the scope of this review. Selected patients may require clearance procedures to measure (rather than estimate) the level of GFR (Table 52).
Mild Decrease in GFR
Using prediction equations to estimate GFR is much less precise at the higher range of GFR, such as CKD Stages 1-2. Early glomerular injury may lead to compensatory hypertrophy and hyperfiltration in less affected nephrons, thereby maintaining or increasing GFR. At the upper range of kidney function, the role of the kidney in determining serum creatinine is of comparable magnitude to variation in other factors such as the metabolism of creatine in skeletal muscle and ingested meat in the diet. The degree of creatinine secretion can vary with time, by as much as 10% even within healthy individuals.111 Additionally, with a mild decrease in kidney function, only a slight increase in the serum creatinine may be seen because of an increase in tubular secretion. Therefore, other markers of early kidney damage are needed to identify early decline in kidney function.
Progression of Kidney Disease
Measurement of progression of kidney disease is substantially more difficult than diagnosis of the presence of kidney disease since progression of many forms of kidney disease is slow. Estimates of GFR based on serum creatinine will allow for reliable detection of substantial progression (>25% to 50% decline). However, substantial changes in secretion, generation, and extra-renal metabolism of creatinine can occur and will lead to false measures of lower degrees of progression. It is particularly difficult to use serum creatinine alone to assess progression of kidney disease in children, in whom growth and maturation lead to substantial changes in muscle mass.
Serum creatinine-based estimates of GFR using prediction formulas in adults and children provide a basis for classification of chronic kidney disease and detection of substantial progression. For teenagers and young adults, use of both formulas (Schwartz and MDRD Study) may give the clinician a dependable range of estimates of GFR. In certain clinical situations, clearance measures may be necessary to estimate GFR (Table 52).
All individuals should be informed about their estimated level of GFR. Individuals with an estimated GFR below 60 mL/min/1.73 m2 are classified as having chronic kidney disease and should be educated about their diagnosis and the implications of decreased kidney function.
Individuals with a serum creatinine of 2.0 mg/dL have moderate to severe decrease in GFR, regardless of the equation used to estimate GFR. However, these individuals constitute only a minority of individuals with chronic kidney disease.
Review of the literature showed a paucity of data on the lower limit of a normal GFR in elderly populations. Therefore, older individuals with low GFR should be assessed for other markers of chronic kidney disease including hypertension and proteinuria.
When precise measures of GFR are necessary, or when muscle mass may deviate substantially from values predicted by age, race, sex in adults or height in children (eg, in malnourished patients174,190-193), clearance measures using exogenous filtration markers may be necessary. In patients with mild or moderate decreased GFR, post-cimetidine creatinine clearance may more closely approximate GFR, as cimetidine blocks tubular secretion of creatinine.169,181 There is a growing literature on using serum cystatin C to estimate GFR. However, limited sample size, statistical methodology, lack of information on cystatin C assay calibration, and conflicting results make the available data inadequate for recommending cystatin C measurement for widespread clinical application.116 Non-radiolabeled iothalamate can be used to decrease the cost and inconvenience of measuring GFR.194
Development and implementation of international standardization and calibration of serum creatinine assays will be important in allowing for the accurate diagnosis of mild and moderate kidney disease. The importance of accurate measurement of serum creatinine needs to be recognized by clinical chemistry laboratories and equipment manufacturers.
Estimating GFR
Although existing equations based on serum creatinine provide an excellent cost-effective method for estimating GFR, their precision is limited. New methods are needed, particularly for detecting mild and moderate kidney disease, but their value in terms of bias, precision, and practicality should be well tested in large samples of subjects with and without kidney disease. In adults, new measures will have to perform substantially better than the 12.1% median difference (~90% of estimates within 30%) from GFR obtained with serum creatinine, age, sex, and race using the MDRD Study equation. In children, standardization of creatinine measurement across studies, use of gold standard GFR measures for reference, and inclusion of larger samples of children of different ages and ethnicities will allow refinement of the constants which should be used in estimating GFR in future modifications of the Counahan-Barratt or Schwartz formula.
While the MDRD Study equation has many advantages, it needs further validation. In particular, further studies should focus on individuals with diabetes, mild decreases in kidney function or normal GFR, Mexican-Americans (whose average serum creatinine is lower than Caucasians), and non-US populations. The extent to which averaging multiple estimates improves precision needs further study. Including a direct measure of body composition by bioelectric impedance or dual-energy X-ray absorptiometry scanning may provide promising directions for improving on the prediction of GFR using serum creatinine.
Definition of “Normal” GFR Across Ages and Ethnicities
The definition of decreased GFR relies on an understanding of the “normal” GFR range. The amount of data in healthy individuals of different ethnicities and children is limited. GFR may differ across ethnic groups but data are very sparse. It is also unknown to what extent a mild decrease in GFR among individuals without hypertension is indicative or kidney disease or “normal” aging.
Prediction Equations for Creatinine Excretion
It would be useful in clinical practice to be able to estimate creatinine excretion from physiologic variables related to creatinine generation and extra-renal elimination, such as age, gender, race, body size, and GFR. This might be done in cross-sectional studies that measured these physiologic variables as well as 24-hour urine creatinine excretion. This would allow improved estimates of daily excretion of some urine solutes from measurements of solute-to-creatinine ratio in spot urine samples.

{kind=link}
{kind=link}