GUIDELINE 15. ASSOCIATION OF CHRONIC KIDNEY DISEASE WITH CARDIOVASCULAR DISEASE
Patients with chronic kidney disease, irrespective of diagnosis, are at increased risk of cardiovascular disease (CVD), including coronary heart disease, cerebrovascular disease, peripheral vascular disease, and heart failure. Both “traditional” and “chronic kidney disease related (nontraditional)” CVD risk factors may contribute to this increased risk.
- All patients with chronic kidney disease should be considered in the “highest risk” group for cardiovascular disease, irrespective of levels of traditional CVD risk factors.
- All patients with chronic kidney disease should undergo assessment of CVD risk factors, including:
- Measurement of “traditional” CVD risk factors in all patients;
- Individual decision-making regarding measurement of selected “CKD-related” CVD risk factors in some patients.
- Recommendations for CVD risk factor reduction should take into account the “highest-risk” status of patients with chronic kidney disease.
Similar to the general population, cardiovascular disease accounts for 40% to 50% of all deaths in the end-stage renal disease (ESRD) population, and CVD mortality rates in ESRD patients are approximately 15 times higher than the general population.261 The burden of cardiovascular disease is evident upon the initiation of replacement therapy. Forty percent of patients starting dialysis already have evidence of coronary heart disease (CHD)2 and only 15% are considered to have normal left ventricular structure and function by echocardiographic criteria.620 Clearly, many manifestations of cardiovascular disease arise before the onset of kidney failure and the need for dialysis or transplantation.
Previously the National Kidney Foundation convened a Task Force to evaluate the epidemic of cardiovascular disease in patients with chronic kidney disease.9 Highlighted in this report was the high mortality from cardiovascular disease in patients with kidney failure. The purpose of this guideline is to focus on the CVD risk associated with chronic kidney disease (excluding patients treated by dialysis). Guideline 14 addresses the risk of cardiovascular disease in patients with diabetic kidney disease. Therefore, this guideline focuses on the risk of cardiovascular disease in patients with nondiabetic kidney disease, and specifically to address the question whether chronic kidney disease is a risk factor for the development of cardiovascular disease. Guidelines for the evaluation and management of specific CVD risk factors in this population are currently being developed by other KDOQI Work Groups.
Definitions
For the purposes of this guideline, “cardiovascular disease” refers to coronary heart disease, cerebrovascular disease, peripheral vascular disease, and congestive heart failure. Left ventricular hypertrophy (LVH) was not always included, even though it is associated with chronic kidney disease and is a risk factor for clinical cardiovascular events. “Traditional” risk factors are those variables defined in the general population through prospective cohort studies such as the Framingham Heart Study (Table 130).
“Chronic kidney disease (CKD)-related” risk factors include the hemodynamic and metabolic abnormalities associated with chronic kidney disease and complications of decreased kidney function. Some authors have subdivided CKD-related risk factors in those factors altered by the “uremic” state (for example, hypertension, dyslipidemia, homocysteine) and factors that are characteristic of the “uremic” state (for example, anemia, malnutrition, oxidative stress, and hyperparathyroidism).621
Strength of Evidence
Where possible, data from the NKF Task Force on Cardiovascular Disease in Chronic Renal Disease9 has been used as the source of information for this guideline. Given the breadth of the topic and the extensive summary by the NKF Task Force, the current Work Group did not feel it was necessary to duplicate their effort. In addition to the Task Force summary, other recent review articles, where necessary, were used as a source of information for the following rationale statements. To determine the association of albuminuria and decreased GFR with incident cardiovascular disease, evidence tables were compiled after a systematic review of original articles.
Nondiabetic patients with chronic kidney disease have an increased prevalence of cardiovascular disease compared to the general population (R). Highlighted in the NKF Task Force Report was the high prevalence of cardiovascular disease in dialysis patients.9 Data from the USRDS in 1997 show a 40% prevalence of either coronary artery disease or congestive heart failure in patients starting dialysis.2 However, few studies have examined the prevalence of cardiovascular disease in a representative sample of patients with earlier stages of chronic kidney disease. In a report from the Framingham Heart Study, the prevalence of various manifestations of cardiovascular disease were examined in participants with elevated serum creatinine (serum creatinine 1.5 to 3.0 mg/dL and 1.4 to 3.0 mg/dL in men and women, respectively). In men, CVD prevalence was 17.9% and in women, CVD prevalence was 20.4%. This contrasts with the CVD prevalence reported in the same study in men (13.9%) and women (9.3%) with normal serum creatinine levels.622 In another cross-sectional analysis, the prevalence of LVH by echocardiography was 27%, 31%, and 45% in patients with a creatinine clearance greater than 50, 25 to 50, and less than 25, respectively.257 This high prevalence of LVH contrasts with a prevalence of less than 20% in Framingham Heart Study participants.623
Cardiovascular disease is the leading cause of death in nondiabetic patients with chronic kidney disease (R). disease is the leading cause of death in patients with chronic kidney disease, regardless of stage of kidney disease. Approximately 40% of all deaths in the United States are secondary to cardiovascular disease.624 Studies involving patients with kidney disease are not dissimilar. In an ancillary analysis of the Hypertension Detection and Follow-up Program (HDFP) involving nearly 11,000 individuals, 58% of deaths in participants with baseline serum creatinine ≥ 1.7 mg/dL were secondary to cardiovascular causes.510 In the British Regional Heart Study comprising 7690 men followed for more than 14 years, greater than 50% of all deaths in subjects within the upper decile of baseline serum creatinine were secondary to cardiovascular causes.625 Although the HDFP and British Regional Heart Study analyses did not stratify by diabetes status, only a minority of subjects was known to be diabetic (16% within the HDFP study and <2.0% within the British Regional Heart Study).
Cardiovascular disease mortality is more likely than development of kidney failure in nondiabetic patients with chronic kidney disease (R). Most patients with chronic kidney disease do not develop kidney failure. The prevalence of chronic kidney disease by stage is shown in Table 4. The estimated prevalence of Stage 3 CKD is ~30 times greater than the prevalence of kidney failure (Stage 5 CKD). Although no prospective data on a cohort with Stage 3 CKD is available, indirectly it is evident that most of these individuals do not proceed to kidney failure, but likely die before the onset of kidney failure. From the discussion above, the cause of death is likely cardiovascular in origin. Further supportive data is available from the HDFP and Framingham analyses. In the HDFP trial, only 19% of deaths were attributable to kidney failure versus 58% from cardiovascular causes.510 In the Framingham study, 198 deaths occurred in subjects with elevated serum creatinine values.622 Only 10 of these deaths occurred when patients had already developed ESRD (unpublished data).
Nondiabetic patients with chronic kidney disease have an increased prevalence of “traditional” CVD risk factors compared to the general population (R).
Prevalence of risk factors with decreased GFR. Many patients with chronic kidney disease have a higher prevalence of traditional CVD risk factors compared to the general population. Data from NHANES III (Table 26) clearly illustrate the inverse association between older age and reduced GFR. Using the same dataset, the prevalence of diabetes and hypertension in subjects with elevated serum creatinine levels (≥1.6 mg/dL in men and ≥1.4 mg/dL in women) in this database was recently reported. In this cross-sectional study, 19% of subjects with elevated serum creatinine were known to have diabetes mellitus, and 70% had high blood pressure. In contrast, the prevalence of diabetes mellitus and hypertension in the entire NHANES III sample was 4.8% and 22.8%, respectively.5 A more extensive discussion on the association of hypertension with GFR is found under Guideline 7. Compared to the general population, the percent prevalence of lipoprotein abnormalities in patients with chronic kidney disease is also increased (Table 131).
The prevalence of tobacco use in patients with chronic kidney disease does not appear to be markedly different from the prevalence in the general population.626
Prevalence of risk factors with proteinuria. Proteinuria is a strong independent predictor of GFR decline in patients with and without diabetes mellitus.6 Therefore, it is not surprising that many of the same CVD risk factors associated with decreased GFR are also associated with increased urinary protein excretion. Proteinuria increases with age and the duration and severity of hypertension.628 In patients with essential hypertension, the combined presence of proteinuria and dyslipidemia is frequent, and greater levels of urinary protein correlate significantly with greater serum levels of total cholesterol, triglycerides, and lipoprotein(a). Proteinuria is also inversely correlated with HDL cholesterol levels.628 The positive correlation between proteinuria and blood pressure, total serum cholesterol, and triglycerides, and the inverse correlation with HDL cholesterol, have also been reported in a recent analysis of data from the MDRD Study.629 These associations remained present even after adjustment for the presence of diabetes. Evidence for abnormalities of the coagulation system with increased fibrinogen, increased von Willebrand factor, and reduced plasminogen activator inhibitor have also been described in patients with elevated levels of urinary protein.630
Nondiabetic patients with chronic kidney disease have a high prevalence of “chronic kidney disease-related” CVD risk factors (R). Numerous hemodynamic and metabolic factors associated with chronic kidney disease have been implicated as potential CVD risk factors (Table 130). The prevalence of many of these factors increases as GFR declines. The inverse association between anemia and GFR is reviewed in Guideline 8. The increased prevalence of abnormalities in PTH, and calcium and phosphate metabolism, are reviewed in Guideline 10. The reader is also referred to reviews which discuss factors such as homocysteine, inflammatory markers, thrombogenic factors, and oxidative stress in more detail.3,631-633
Chronic kidney disease is a risk factor for subsequent cardiovascular disease in individuals without diabetes (C).
Decreased GFR is a risk factor for cardiovascular disease in individuals without diabetes (Tables 132 and 133 and Fig 53) (C).
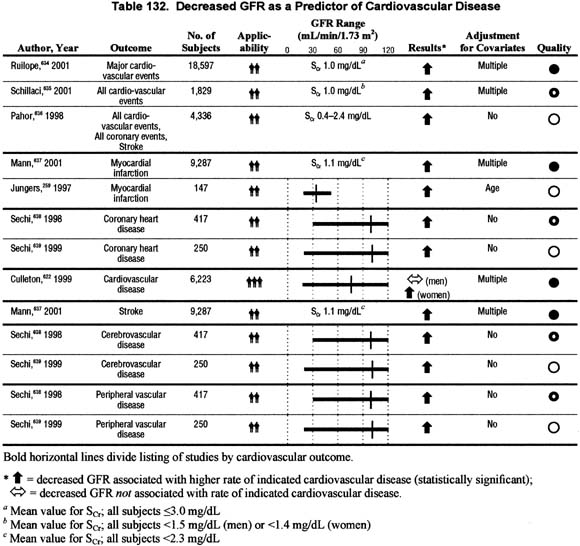
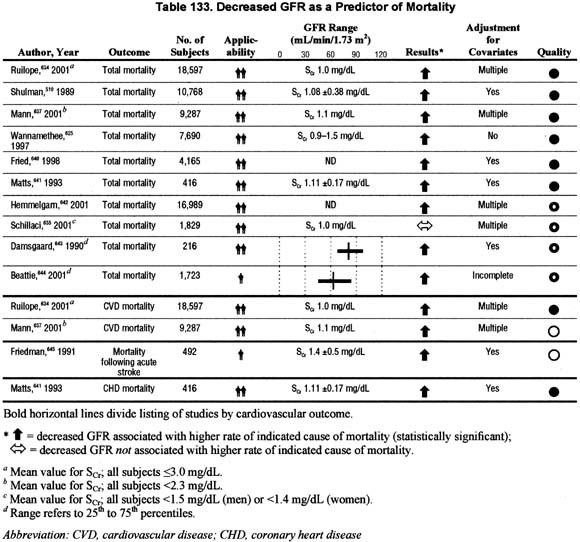
Figure 53 |
|
| GFR and relative risk for death. Wannamethee625: risk is for SCr ≥ 1.5 mg/dL versus SCr |
|
Reduced GFR identifies individuals at greater risk for CVD events, including coronary heart disease, cerebrovascular disease and peripheral vascular disease, and death. The results of these studies are not entirely consistent. Some of this variability may be explained on differences in baseline demographics, severity of kidney disease, and the overall cardiovascular risk of the study sample. There is insufficient evidence to support an association with incident congestive heart failure, possibly because the number of congestive heart failure events is low.
Proteinuria is a risk factor for cardiovascular disease in individuals without diabetes (Tables 134, 135, and 136 and Figs 54, 55, and 56) (C).
Figure 54 |
|
Proteinuria and relative risk for cardiovascular disease. Where possible, results presented are from multivariable analyses. Agewall650, Ljungman647: Unadjusted results shown. Data not available to calculate age or multivariable adjusted risk. |
|
Figure 55 |
|
Proteinuria and relative risk for CVD death. Where possible, results presented are from multivariable analyses. Agewall650: unadjusted results shown. Data not available to calculate age or multivariable adjusted risk. Jager651, Kannel12, Culleton648: some diabetics included, but results shown are adjusted for diabetes. Grimm228: (a) proteinuria positive once; (b) proteinuria positive more than once over 6 years of follow-up. |
|
Figure 56 |
|
Proteinuria and relative risk for death. Where possible, results presented are from multivariable analyses. Damsgaard643 : 4/216 subjects excreted more than 200 µg/min of albumin. Agewall650: unadjusted results shown. Data not available to calculate age or multivariable adjusted risk. Jager651, Kannel12, Culleton648: some diabetics included, but results shown are adjusted for diabetes. Grimm228: (a) proteinuria positive once; (b) proteinuria positive more than once over 6 years of follow-up. Miettinen649: Results not shown. Proteinuria predicted mortality but data was not provided to calculate risk. |
|
Likewise, proteinuria is also a risk factor for CVD events, CVD mortality, and all-cause mortality. Again, the results for all studies are not completely consistent but the weight of evidence is very supportive.
The identification of chronic kidney disease as a risk factor for cardiovascular disease does not prove causation. A temporal relation with chronic kidney disease and incident cardiovascular disease has been identified in many of these studies, but other criteria for causation are lacking, including consistency and biologic plausibility. Furthermore, although a dose-response relationship with proteinuria and cardiovascular disease may exist, such a relationship with reduced GFR has not been shown conclusively. An alternative hypothesis is that chronic kidney disease is a marker for the burden of exposure to “traditional” CVD risk factors. The relative contribution from “kidney disease-related” risk factors in this population remains uncertain.
Risk factor reduction is likely to be effective in reducing morbidity and mortality due to cardiovascular disease in patients with chronic kidney disease (O). Few patients with chronic kidney disease have been included in clinical trials with “hard” cardiovascular endpoints. In the absence of this high level evidence, extrapolation of evidence from clinical trial results in the general population to patients with chronic kidney disease is necessary. Several lines of reasoning support this process. First, “traditional” CVD risk factors can be modified in patients with chronic kidney disease. Clearly, antihypertensive agents are effective in lowering blood pressure. Lipid parameters can be improved with dietary and pharmacologic therapy. Smoking cessation programs should be no less effective in patients with chronic kidney disease than in the general population.
Second, adverse effects of risk factor reduction do not appear substantially greater in patients with chronic kidney disease than in the general population.
Third, the life span of most patients with chronic kidney disease often exceeds the duration of treatment required for beneficial effects. In the general population, the beneficial effect of risk factor reduction on morbidity and mortality begins to appear within 1 to 3 years or less in high risk groups. For example, survival curves for high risk patients randomized to lipid lowering therapy frequently diverge from placebo treated patients within 6 months of the start of treatment. The life-span of most patients with chronic kidney disease exceeds 1 to 3 years.
Treatment recommendations are beyond the scope of this guideline. The reader is referred to the NKF Task Force Report9 for a summary of treatment recommendations for traditional CVD risk factors in chronic kidney disease, and to forthcoming KDOQI guidelines on CKD-related CVD risk factors.
The variety of measures used to assess kidney function has placed a significant limitation on this current review. This is particularly true for the assessment of CVD risk associated with reduced GFR. As a marker for GFR, serum creatinine was used in most studies. The limitations with serum creatinine measurements have been described previously. Few studies provided data on creatinine clearance, and no prospective studies provided a more accurate measure of GFR than serum creatinine. As a result, it was not possible to quantify the prevalence of cardiovascular disease or CVD risk factors by stage of kidney disease. Furthermore, the risk for future CVD events could not be defined by stage of kidney disease. A similar problem was found during the assessment of CVD risk associated with albuminuria. Older studies used dipsticks on random urines. Some dipsticks measured total protein, while others measured albumin excretion. More recent studies have quantified albumin excretion with more standardized techniques. The variability in urine protein measurement makes comparisons between studies difficult.
In addition, few studies provided analyses stratified by diabetes status. In contrast to the literature on CVD risk in diabetic kidney disease, few generalizable studies have been published on CVD risk specifically in nondiabetic individuals with chronic kidney disease. To our advantage, many of the studies reviewed included less than 10% diabetic patients. The Work Group agreed to extrapolate results from these mixed samples, limiting assessments to qualitative statements.
“Traditional” CVD risk factors appear to be shared risk factors for both chronic kidney disease and cardiovascular disease and therefore are in high prevalence in chronic kidney disease. Therefore, it is essential to develop interdisciplinary programs for detection and treatment of traditional risk factors, emphasizing the inter-relationships among diabetes, cardiovascular disease, and kidney disease.
Physician, allied health, and patient education initiatives are necessary to ensure that patients with chronic kidney disease are recognized to be at high risk for future CVD events, irrespective of diagnosis. Coordinated patient management systems will be necessary to appropriately recognize and manage CVD risk factors in this patient population.
A large prospective multi-ethnic cohort study involving patients with Stage 3 and 4 chronic kidney disease is necessary to further examine the impact of “traditional” and “kidney disease-related” risk factors on incident cardiovascular disease. Emphasis should be placed on the recognition of potentially modifiable risk factors. Such a study could also determine the time course of cardiovascular disease in the chronic kidney disease population.
A predictive clinical tool, using kidney disease stage and diagnosis, risk factors, and/or other variables, should be developed to better predict risk in patients with chronic kidney disease.
Standards for the measurement of kidney function and albuminuria in observational and controlled trials should be established.
{kind=link}
{kind=link}