GUIDELINE 2. EVALUATION AND TREATMENT
The evaluation and treatment of patients with chronic kidney disease requires understanding of separate but related concepts of diagnosis, comorbid conditions, severity of disease, complications of disease, and risks for loss of kidney function and cardiovascular disease.
- Patients with chronic kidney disease should be evaluated to determine:
- Diagnosis (type of kidney disease);
- Comorbid conditions;
- Severity, assessed by level of kidney function;
- Complications, related to level of kidney function;
- Risk for loss of kidney function;
- Risk for cardiovascular disease.
- Treatment of chronic kidney disease should include:
- Specific therapy, based on diagnosis;
- Evaluation and management of comorbid conditions;
- Slowing the loss of kidney function;
- Prevention and treatment of cardiovascular disease;
- Prevention and treatment of complications of decreased kidney function;
- Preparation for kidney failure and kidney replacement therapy;
- Replacement of kidney function by dialysis and transplantation, if signs and symptoms of uremia are present.
- A clinical action plan should be developed for each patient, based on the stage of disease as defined by the KDOQI CKD classification (see Table 33).
- Review of medications should be performed at all visits for the following:
- Dosage adjustment based on level of kidney function;
- Detection of potentially adverse effects on kidney function or complications of chronic kidney disease;
- Detection of drug interactions;
- Therapeutic drug monitoring, if possible.
- Self-management behaviors should be incorporated into the treatment plan at all stages of chronic kidney disease.
- Patients with chronic kidney disease should be referred to a specialist for consultation and co-management if the clinical action plan cannot be prepared, the prescribed evaluation of the patient cannot be carried out, or the recommended treatment cannot be carried out. In general, patients with GFR <30 mL/min/1.73 m2 should be referred to a nephrologist.
Historically, the evaluation and management of chronic kidney disease has focused on diagnosis and treatment of specific kidney diseases and dialysis or transplantation for kidney failure. An action plan for patients with chronic kidney disease also requires interventions during the earlier stages of kidney disease, irrespective of the cause of kidney disease. This includes evaluation and management of comorbid conditions, slowing progression of kidney disease, cardiovascular disease risk reduction, preventing and treating complications of chronic kidney disease, and preparation for kidney replacement therapy.
Diagnosis (R, O). Classification of the type of kidney disease is based on pathology and etiology. A simplified classification, and the distribution of types of kidney disease leading to ESRD are given in Table 34.
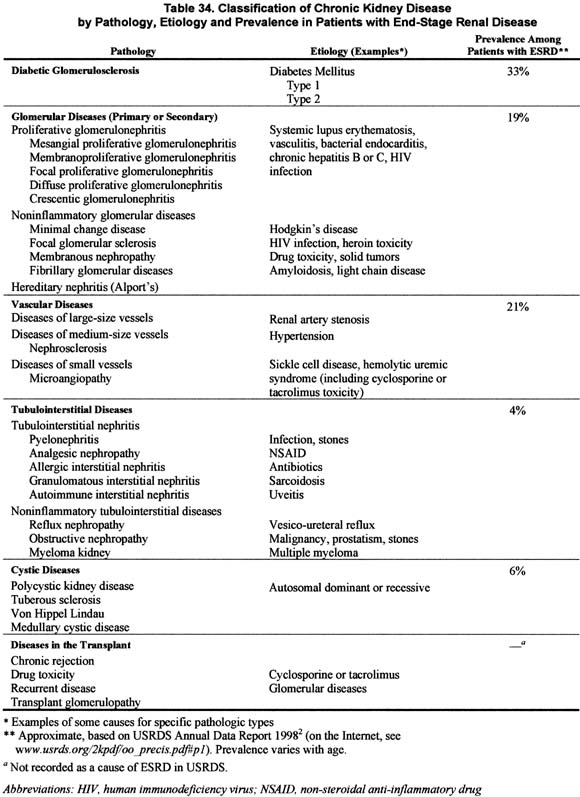
The definitive diagnosis of the type of kidney disease is based on biopsy or imaging studies. Biopsy and invasive imaging procedures are associated with a risk, albeit usually small, of serious complications. Therefore, these procedures are often avoided unless a definitive diagnosis would change either the treatment or prognosis. In most patients, well-defined clinical presentations and causal factors provide a sufficient basis to assign a diagnosis of chronic kidney disease. An approach to diagnosis, based on concepts elaborated on in this report, is given in Part 9.
Diabetic kidney disease is a type of glomerular disease, but it is singled out here because it is the largest single cause of kidney failure. Both type 1 and type 2 diabetes cause chronic kidney disease. Because of the higher prevalence of type 2 diabetes, it is the more common cause of diabetic kidney disease. The clinical features, natural history and treatment for diabetic kidney disease are well known because it has been the subject of numerous epidemiological studies and clinical trials. Diabetic kidney disease usually follows a characteristic clinical course after the onset of diabetes, first manifested by microalbuminuria, then clinical proteinuria, hypertension, and declining GFR. Clinical trials have established a number of effective treatments to slow the development and progression of diabetic kidney disease, including strict glycemic control, angiotensin-converting enzyme inhibitors and angiotensin receptor blockers, blood pressure control, and perhaps dietary protein restriction.
A variety of diseases, including other glomerular diseases, vascular diseases, tubulointerstitial diseases, and cystic diseases, are often grouped together under the label “nondiabetic kidney diseases” for the purpose of epidemiological studies and clinical trials. Amongst these, hypertensive nephrosclerosis and glomerular diseases are the second and third most common causes of kidney failure. The various diseases in this group differ widely based on history, clinical presentation, risk for progression, and response to treatment. Differentiation among the diseases can be difficult, often requiring kidney biopsy or invasive imaging studies. An approach to diagnosis, based on the history, and a review of clinical presentations of chronic kidney disease, are given in Part 9. Specific therapies are available to reverse abnormalities in structure and function for some types of chronic kidney disease: for example, immunosuppressive medications for autoimmune glomerular diseases, antibiotics for urinary tract infections, removal of urinary stones, relief of obstruction, and cessation of toxic drugs. A thorough search for “reversible causes” of decreased kidney function should be carried out in each patient with chronic kidney disease.
Kidney disease in the transplant is probably the fourth largest cause of kidney failure. Both immunologic and non-immunologic factors appear to play an important role. The most common causes are chronic rejection, toxicity due to cyclosporine or tacrolimus, recurrent disease, and transplant glomerulopathy. In addition, differential diagnosis includes all the diseases that can occur in the native kidney. For a variety of reasons, especially the ease and safety of kidney biopsy, there is generally a much lower threshold for performing invasive procedures to establish a definitive diagnosis in kidney transplant recipients.
Comorbid conditions (R, O). Patients with chronic kidney disease have a large number of comorbid conditions. Comorbidity is defined as conditions other than the primary disease (in this case, chronic kidney disease). Complications of chronic kidney disease, such as hypertension, anemia, malnutrition, bone disease and neuropathy, are not considered as comorbid conditions. It is useful to consider three types of comorbid conditions (Table 35).
Diseases which cause chronic kidney disease. Evaluation and management of these diseases is important for patients’ well being and may improve the course of chronic kidney disease. This is particularly important for patients with diabetes and high blood pressure, the leading causes of chronic kidney disease and cardiovascular disease in the United States.
Unrelated diseases, which may lead to impairments of functioning and well being but do not affect the course of chronic kidney disease. Evaluation and management is important for patients’ health and well being.
Cardiovascular disease. Cardiovascular disease is singled out from among the possible comorbid conditions to emphasize its complex relationship with chronic kidney disease, and its importance as a preventable cause of morbidity and mortality in patients with chronic kidney disease.
In all cases, management of comorbid conditions must be integrated into the overall care of patients with chronic kidney disease. Examples include adjustment of drug dosages, interpretation of symptoms, and minimizing treatment complications, including acute decline in kidney function. In patients with normal or mildly decreased GFR (CKD Stages 1-2), integration of care for chronic kidney disease and these comorbid conditions may be relatively simple. However, in patients with moderate to severe reduction in GFR (CKD Stages 3-4) and in patients with kidney failure (CKD Stage 5), integration of care is complex and requires careful coordination among all providers.
Risk of loss of GFR (R, O). Risk of kidney failure depends on the level of GFR (severity) at detection of kidney disease and the rate of loss of GFR thereafter. Level of GFR can be improved by specific treatment in some chronic kidney diseases, but not in most others.
Rate of loss of GFR (progression of kidney disease) is affected by diagnosis and by modifiable and nonmodifiable patient factors. These factors can be assessed even before the decline in GFR, thereby allowing implementation of interventions to slow progression while GFR is still normal. Some therapies to prevent or slow the loss of GFR are specific for the diagnosis, while others are non-specific. Factors associated with progression of kidney disease are discussed in Guideline 13.
It is difficult to estimate the rate of progression until there has been a decline in GFR. In diseases characterized by a quantifiable marker of damage—for example, albuminuria in diabetic kidney disease—progression, stability, or regression can be estimated by change in the marker. For most diseases, however, quantitative relationships between changes in markers and progression have not been established.
Severity of disease and complications (R, O). Decreased GFR is associated with a wide range of complications due to disorders in other organ systems, which are manifested by hypertension, laboratory abnormalities, and symptoms. Complications due to disorders in other organ systems are associated with worse outcomes. Early detection and treatment of complications can improve outcomes. The prevalence of complications of chronic kidney disease is mainly related to the level of GFR. Interpretation of signs and symptoms in patients with chronic kidney disease should be guided by the level of GFR.
Kidney functions other than GFR may be altered by chronic kidney disease. These include maintenance of the filtration barrier for plasma proteins (abnormalities include albuminuria and proteinuria), reabsorption or secretion of water or specific solutes (abnormalities include tubular syndromes), and various endocrine functions (erythropoietin deficiency causes anemia, parathyroid hormone excess causes bone disease, and vitamin D deficiency causes bone disease). For most chronic kidney diseases, severity in other abnormalities of function parallels the severity of decreased GFR. Prevention and treatment of complications of chronic kidney disease includes specific therapies related to the pathogenesis of complications—for example, erythropoietin for anemia and vitamin D for bone disease.
Table 36 shows the association of levels of GFR with complications of chronic kidney disease. Patients with GFR 60 to 89 mL/min/1.73 m2 usually have hypertension and may have laboratory abnormalities indicative of dysfunction in other organ systems, but usually no symptoms. Patients with GFR 30 to 59 mL/min/1.73 m2 have laboratory abnormalities in several other organ systems, but few symptoms. Patients with GFR 15 to 29 mL/min/1.73 m2 usually have laboratory abnormalities in many organ systems and have mild symptoms. Patients with GFR <15 mL/min/1.73 m2 usually have many symptoms and laboratory abnormalities in several organ systems, collectively known as the “uremic syndrome.” The association of complications of chronic kidney disease with the level of GFR is discussed in Part 6, Guidelines 7 through 12.
Risk of cardiovascular disease (R, O). Cardiovascular disease may be a cause and complication of chronic kidney disease. Irrespective of diagnosis, the increased risk of cardiovascular disease in individuals with chronic kidney disease can be attributed to: (1) a higher prevalence of “traditional” CVD risk factors; and (2) risk factors related to the hemodynamic and metabolic complications of chronic kidney disease (“CKD-related” or “nontraditional” CVD risk factors). Treatment and prevention of cardiovascular disease in chronic kidney disease includes risk factor reduction as well as specific therapies for cardiovascular disease and should begin as early as possible. CVD risk factors may become more prevalent or more severe as GFR declines; therefore, as GFR declines, treatment must intensify. Cardiovascular disease in chronic kidney disease is discussed in Guideline 15.
Kidney replacement therapy for uremia (R, O). Signs and symptoms of severe decrease in GFR, collectively, are known as “uremia” or the “uremic syndrome.” Replacement therapy (dialysis and transplantation) is effective in improving the most serious features of uremia, irrespective of the type of chronic kidney disease. Patients require education and advance preparation to cope with the stresses of kidney failure, to choose a modality of kidney replacement therapy, and to undergo evaluation for that modality. It is recommended that preparation for kidney replacement therapy begin when GFR declines below 30 mL/min/1.73 m2. All patients should probably be instructed to preserve suitable veins for possible future vascular access construction. The indications for initiation of kidney replacement therapy are based on the level of kidney function and presence of signs and symptoms of uremia. Most individuals begin dialysis or receive a kidney transplant when GFR is less than 15 mL/min/1.73 m2.
Drug prescribing in chronic kidney disease (R). Patients with chronic kidney disease are prescribed a large number of medications. In addition, patients may take other medications, such as over-the-counter medications, “non-traditional” medications, vitamins and supplements, herbs, and drugs of abuse. A thorough review of the medication list and all other medications should be conducted at each visit. Drug dosage should be adjusted for the level of estimated GFR. Drugs with potentially adverse effects on kidney function or complications of decreased kidney function should be discontinued if possible. Drug-drug interactions should be considered. Because of possible alterations in volume of distribution, protein binding, drug elimination, and drug-drug interactions in chronic kidney disease, therapeutic drug monitoring should be performed, if possible. A large amount of information is available to providers in texts, manuals, and databases for handheld computers. Interpretation may be facilitated by the similarity between the classification of levels of kidney function proposed in this guideline and the recommendations for pharmacokinetic studies of drugs in patients with decreased kidney function made by the Food and Drug Administration84 (on the Internet, http://www.fda.gov/cder/guidance/1449fnl.pdf).
Barriers to adherence in chronic kidney disease (R, O). Healthy people make choices that could ultimately shorten their lives, such as smoking, drinking or eating too much, not exercising, missing prescribed medications, and failing to get an annual physical. Those with chronic health conditions requiring lifestyle changes and clinician-initiated visits are more likely to be noncompliant.85 Patients with chronic kidney disease live day-to-day with such a chronic condition. Other factors linked with noncompliance are shown in Table 37.85-98
Because the terminology “noncompliance” or “nonadherence” often leads to prejudice and negative stereotyping, it is recommended that “self-management behaviors” be substituted.99 The Work Group recommends assessment of barriers to adherence in all patients with chronic kidney disease and incorporation of self-management behaviors into the treatment plan at all stages.
Referral to specialists (O). Frequently the primary care provider will make the diagnosis of chronic kidney disease. Referral to a nephrologist or other specialist for consultation or co-management should be made after diagnosis under the following circumstances: a clinical action plan cannot be prepared based on the stage of the disease, the prescribed evaluation of the patient cannot be carried out, or the recommended treatment cannot be carried out. These activities may not be possible either because the appropriate tools are not available or because the primary care physician does not have the time or information needed to do so. In general, patients with GFR <30 mL/min/1.73 m2 (CKD Stages 4-5) should be referred to a nephrologist.
This guideline provides a conceptual framework to the evaluation and management of chronic kidney disease, but does not provide sufficient details to guide health care providers in the management of individual patients with chronic kidney disease or the design of public policy to improve outcomes for the target population. Subsequent guidelines will elaborate on the concepts in this guideline, but it is beyond the scope of these guidelines to provide specific instructions for evaluation and management. This will be the topic of forthcoming KDOQI guidelines and guidelines by other organizations. The ultimate goal is to develop specific guidelines for each action at each stage of disease.
Almost all aspects of the evaluation and management of chronic kidney disease in textbooks of nephrology could be re-written to incorporate the stages of chronic kidney disease proposed in this guideline. Part 9 provides an approach to selected topics using this classification.
Development of a clinical action plan for all patients with chronic kidney disease is an enormous undertaking that will require coordinate effort of many government and non-governmental organizations. The National Institute of Diabetes, Digestive and Kidney Disease (NIDDK) has established a National Kidney Disease Education Program. The NKF is committed to developing an implementation plan for the KDOQI CKD guidelines and to working with the NIDDK and other organizations to develop a national program.
Much research is needed to define diagnostic and therapeutic strategies to reduce adverse outcomes of chronic kidney disease at each stage of disease. It will also be important to assess the effect of implementing these guidelines on the outcomes of chronic kidney disease.