In CKD Patients (Stages 3 and 4):
7.1 If plasma intact PTH is above the target range for the stage of CKD (Table 15, Guideline 1) serum 25-hydroxyvitamin D should be measured at first encounter. If it is normal, repeat annually. (EVIDENCE)
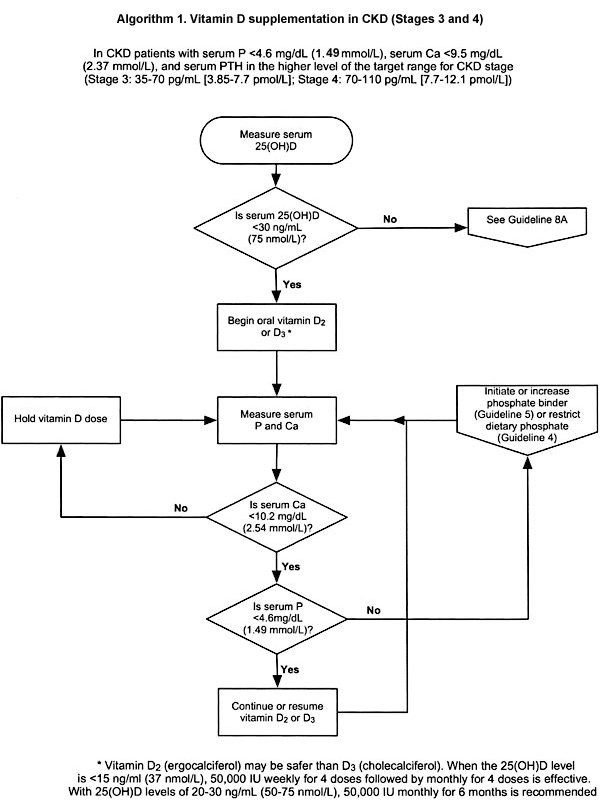
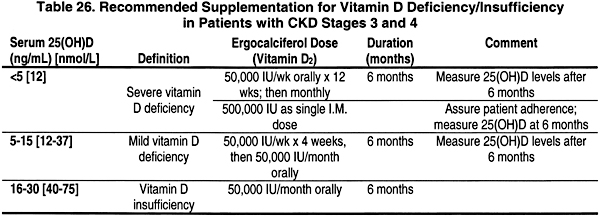
7.2 If the serum level of 25-hydroxyvitamin D is <30 ng/mL (75 nmol/L), supplementation with vitamin D2, (ergocalciferol) should be initiated (Table 26). (OPINION)
7.3 Following initiation of vitamin D therapy:
7.3a The use of ergocalciferol therapy should be integrated with the serum calcium and phosphorus (Algorithm 1).
7.3b The serum levels of corrected total calcium and phosphorus should be measured at least every 3 months. (OPINION)
7.3c If the serum levels of corrected total calcium exceeds 10.2 mg/dL (2.54 mmol/L), discontinue ergocalciferol therapy and all forms of vitamin D therapy. (OPINION)
7.3d If the serum phosphorus exceeds 4.6 mg/dL (1.49 mmol/L), add or increase the dose of phosphate binder. (See Guidelines 4 and 5) If hyperphosphatemia persists, discontinue vitamin D therapy. (OPINION)
7.3e Once patients are replete with vitamin D, continued supplementation with a vitamin-D-containing multi-vitamin preparation should be used with annual reassessment of serum levels of 25-hydroxyvitamin D, and the continued assessment of corrected total calcium and phosphorus every 3 months. (OPINION)
In CKD Patients With Kidney Failure (Stage 5):
7.4 Therapy with an active vitamin D sterol (calcitriol, alfacalcidol, paricalcitol, or doxercalciferol) should be provided if the plasma levels of intact PTH are > 300 g/mL. (OPINION) See Guideline 8B.
Algorithm 1. Vitamin D supplementation in CKD (Stages 3 and 4).
Serum levels of 25-hydroxyvitamin D (not the levels of 1,25-dihydroxyvitamin D) are the measure of body stores of vitamin D. In normal individuals over age 60, levels of 25-hydroxyvitamin D below the "normal" limit of 15 ng/mL and also low to normal levels of 16 to 32 ng/mL are both associated with increased PTH levels, reduced bone mineral density (BMD), and increased rates of hip fracture. Such levels of 25(OH)D are common in patients with CKD and GFR of 20 to 60 mL/min/1.73 m2, and in CKD patients undergoing dialysis. The prevention and treatment of vitamin D insufficiency in patients with CKD Stages 3 and 4 most certainly reduce the frequency and severity of secondary hyperparathyroidism. In patients with more advanced CKD (Stage 5) and in dialysis patients, it is not established that nutritional "replacement" with vitamin D (ergocalciferol or cholecalciferol) will be effective since the ability to generate adequate levels of 1,25(OH)2D3 is markedly reduced or is unlikely.
A reduction of serum 25-hydroxyvitamin D, the substrate for the kidney’s generation of calcitriol [1,25(OH)2D3], produces secondary hyperparathyroidism (2°HPT) in individuals with normal kidney function,212-214 and may aggravate 2°HPT in those with CKD and decreased kidney function.215,216 Severe vitamin D deficiency, with osteomalacia and hypocalcemia, is rare unless 25-hydroxyvitamin D levels are <5 ng/mL (12 nmol/L); however, levels below 30 ng/mL are indications of vitamin D "insufficiency,"217 as manifested by significant elevations of serum levels of intact PTH.217,218 "Normal" individuals with low "normal" 25-hydroxyvitamin D levels of 16 to 32 ng/mL (40 to 80 nmol/L) have lower bone mineral density214; also, patients with hip fractures have lower 25(OH)D levels than age-matched patients without hip fracture.219 The only real disagreement is the upper range of 25(OH)D levels at which one does not encounter significant numbers of patients with secondary hyperparathyroidism,217 indicating that 25(OH)D should be maintained at higher levels.
Studies of 25-hydroxyvitamin D levels in patients with CKD and varying degrees of decreased kidney function from 4 reports were reviewed.45,63,65,220 Among 63 non-nephrotic CKD patients, the median values of 25(OH)D levels in those with GFR of 60 to 90, 40 to 60, and 20 to 40 mL/min/1.73 m2 were 12, 19, and 18 ng/mL (30, 47, and 45 nmol/L), respectively.45 Obviously, a high fraction of these patients had levels below 30 ng/mL (75 nmol/L) and many were below 16 ng/mL (40 nmol/L). In a report of 76 CKD patients, 37 had CKD due to diabetes and 39 from other causes.63 The 25(OH)D level averaged 22.3 ± 9.4 ng/mL (56 ± 23 nmol/L) in nondiabetics and 11.4 ± 5.6 ng/mL (28 ± 14 nmol/L) in the diabetic patients; in the diabetics, serum albumin levels were lower and 76% had urinary protein concentrations above 300 mg/dL compared to 23% of nondiabetics.63 For the total group with GFR of 20 to 50 mL/min/1.73 m2, 47% had 25(OH)D levels below 16 ng/mL (40 nmol/L) and 76% had 25(OH)D levels below 26 ng/mL (65 nmol/L). In these 2 studies,45,63 serum 1,25(OH)2D levels correlated with 25(OH)D levels [r = 0.5145 and r = 0.4763], and P < 0.001. In the third study of the 19 CKD patients with GFR of 20 to 90 mL/min/1.73 m2, 79% had 25(OH)D levels below 26 ng/mL (65 nmol/L) and 18% had 25(OH)D levels below 16 pg/mL (0.4 nmol/L). In a US study that included 9 CKD patients with GFR of 12 to 60 mL/min/1.73 m2, 25(OH)D levels averaged 20 ± 6 ng/mL (50 ± 15 nmol/L) indicating that values were below 30 ng/mL (75 nmol/L) in the majority of patients. The findings that 1,25(OH)2D levels correlated with 25(OH)D levels in the 2 largest series45,63 differ from observations in the normal population, where 1,25(OH)2D levels are not dependent on the 25(OH)D levels, even in patients with vitamin D deficiency.221 The normal, highly efficient production of 1,25(OH)2D by the kidneys when the supply of 25(OH)D is markedly reduced is altered in CKD, and the data indicate that 1,25(OH)2D levels may be more dependent on the availability of 25(OH)D in CKD patients with impaired kidney function.
Patients with CKD or those who are dialysis-dependent are much more likely to have low levels of 25(OH)D in comparison to those with no kidney disease for several reasons:
(1) Many are inactive with reduced exposure to sunlight.
(2) The ingestion of foods that are natural sources of vitamin D (fish, cream, milk, and butter) is likely to be lower than in the normal population;
(3) Serum 25-hydroxyvitamin D levels may be subnormal in CKD patients because the endogenous synthesis of vitamin D3 in the skin following identical exposure to sunlight is reduced in those with reduced GFR,222 in individuals over age 60,223 and in individuals with increased melanin content of the skin.224
The ingestion of a diet low in calcium content leads to greater conversion of 25-hydroxyvitamin D to calcitriol and the need for more vitamin D intake and/or production,225 and dietary calcium intake is frequently low in CKD patients.195 Furthermore, there is increased need for vitamin D in CKD patients with nephrotic-range proteinuria, because urinary losses of 25-hydroxyvitamin D and vitamin D-binding protein (DBP) are high.220,226 Kidney disease was found to be a major risk factor for low plasma 25-hydroxyvitamin D levels in a population study of patients hospitalized in New England (with patients on dialysis excluded from the analysis).218
In countries such as the United States where many foods are supplemented with vitamin D, and others such as Japan and the Scandinavian countries, where fish intake is high, the incidence of vitamin D insufficiency is lower than in European countries of similar latitudes but where fish intake is low and vitamin-D-supplemented foods are unavailable.217 Nonetheless, 14% to 42% of apparently healthy individuals, over age 60, in the United States had plasma levels of 25(OH)D below 24 or 25 ng/mL (60 or 62 nmol/L).227,228
In patients with kidney failure (Stage 5) and in those on dialysis, there may be less need for vitamin D as there is little or no generation of calcitriol by the kidneys. However, the data show that 25(OH)D levels below 15 ng/mL (37 nmol/L) are associated with a greater severity of secondary hyperparathyroidism even in CKD patients on dialysis.229 Nonetheless, the value of supplementation with ergocalciferol with these patients is less certain; although in dialysis-dependent patients, including anephric individuals, high doses of ergocalciferol or 25-hydroxyvitamin D can raise the serum levels of calcitriol.230-232
In patients with CKD and GFR of 20 to 60 mL/min/1.73 m2, nutritional vitamin D deficiency and insufficiency can both be prevented by supplementation with vitamin D2 (ergocalciferol) or vitamin D3 (cholecalciferol). If there is evidence of true vitamin D deficiency, this should be treated, and the best available treatment is vitamin D2, although the doses needed are larger than those needed for vitamin D insufficiency. For the prevention of vitamin D deficiency, the recommended daily allowance for vitamin D in individuals over 60 years is 800 IU, and for younger adults 400 IU.
There are problems with the dosage forms available. In the United States, the only forms available are 400 IU (over the counter) and capsules containing 50,000 IU, requiring a prescription. In normal individuals, the recommended upper limit of vitamin D is 2,000 IU/day according to the Food and Nutrition Board, National Research Council, National Academy of Sciences.233,234 This dose can be achieved by giving 1 capsule (50,000 IU) once a month.235,236 Dosage preparations of 10,000 IU of ergocalciferol have been given daily to French patients with advanced CKD for periods longer than 1 year, with no evidence of vitamin D overload or renal toxicity.237,238 The safer vitamin D sterol may be ergocalciferol rather than cholecalciferol,239,240 although there are no controlled comparisons of cholecalciferol and ergocalciferol in humans, and the available commercial preparations employ ergocalciferol (as Calciferol™ or Drisdol™). Calcitriol or another 1a-hydroxylated vitamin D sterol should not be used to treat vitamin D deficiency. When evidence of severe vitamin D deficiency is found, with 25(OH)D levels <5 ng/mL (12 nmol/L), rickets or osteomalacia may be present; treatment can be given using ergocalciferol, 50,000 IU given weekly for 12 weeks and monthly thereafter (see Table 26).236
There is strong evidence that vitamin D insufficiency, defined as 25-hydroxyvitamin D levels below 27 to 32 ng/mL (67 to 80 nmol/L), is common in individuals over 60 years in the United States,227,228 and many locations in Europe.241 Such low levels have clinical significance based on the finding of (1) the elevated serum levels of intact PTH as evidence of secondary hyperparathyroidism; and (2) reduced BMD214 and higher rates of hip fracture compared to age-matched controls.242 The clinical significance of this is further demonstrated by data showing that supplementation with vitamin D, 800 IU/day, along with a modest dietary calcium supplement reduced hip fracture rate by 43% in a double-blinded, placebo-controlled trial.241,243 There have been reports in patients with CKD that suggest there may be adverse clinical consequences of suboptimal serum levels of 25(OH)D, including the finding that 25-hydroxyvitamin D levels below 15 ng/mL pose a major risk factor for the presence of severe secondary hyperparathyroidism (with radiographic abnormalities) in CKD patients on dialysis,229 although the dialysis dose provided to the patients in this study was suboptimal. A substantial prevalence of suboptimal levels of 25(OH)D in CKD patients with GFR of 20 to 60 mL/min/1.73 m2 has been identified in every study of such patients, but the number of individuals studied has been small. Regarding safety, the experience with ergocalciferol doses of 10,000 IU/day237,238 indicates a recommended dose of 1,000 to 2,000 IU/day would be safe.
In patients with GFR <20 mL/min/1.73 m2 and those requiring dialysis, there is no evidence that modest supplementation with ergocalciferol to raise serum 25-hydroxyvitamin D levels to 30 to 60 pg/mL (8.25 to 16.5 pmol/L) will increase the plasma levels of 1,25-dihydroxyvitamin D (calcitriol) or lower the elevated serum levels of intact PTH. In CKD patients with higher GFRs, there is a strong probability that such treatment would have benefit, although there are no data to support this view. One study demonstrated that serum 1,25(OH)2D levels were increased in patients with CKD and moderate kidney failure following the administration of a low-calcium diet, indicating that there is some "reserve" for the generation of 1,25(OH)2D in such patients.244
The treatment of vitamin D insufficiency or deficiency when present in CKD patients is warranted since such therapy may reduce or prevent secondary hyperparathyroidism in the early stages of CKD, and decrease the incidence of hip fractures in patients with advanced CKD and in those treated with dialysis.
Prospective, controlled clinical trials with the daily administration of ergocalciferol in a monthly amount equivalent to 1,000 to 2,000 IU/day, are clearly warranted in patients with CKD and those undergoing dialysis, to assess the effects on serum levels of intact PTH, serum 1,25(OH)2D levels, and even BMD. With the higher fracture rates known to occur in patients with Stage 5 CKD,76 studies to evaluate measures to minimize early secondary hyperparathyroidism would be warranted.